|
Southeast Texas Medical Associates, LLP’s seven-part syllabus for the Medical Student Fourth Year (MS4) Patient-Centered Medical Home (PC-MH) Selective is outlined and described below. The syllabus reflects only a portion of SETMA’s electronic medical record tools, presentations, awards, articles, history and patient-centered-medical-home work. All of our work is detailed at www.jameslhollymd.com particular under Your Life Your Health, Presentations, In-the-News, Public Reporting, and Medical Home.
We often refer to ourselves as the “healthcare exhibitionists”: If we have done it; it is on our website. Our work includes association with the Diabetes Center of Excellence, the Robert Wood Johnson Foundation, the Institute for Healthcare Improvement, the Office of National Coordinator (ONC) of Health Information Technology (HIT), the Agency for Healthcare Research and Quality, the American Board of Family Practice, the Physician Consortium for Performance Improve, the National Quality Forum, the Johnson and Johnson Company, IBM, HIMSS and numerous other organizations.
Ten years ago, SETMA was asked to define our ultimate goal in practice. With humility and recognition of our limitations in this regard, we cautiously said, “Our goal is to help change how healthcare is delivered in America.” Through our transformative use of electronic medical records, morphed into electronic patient management, and our adoption of patient-centered medical home, we hopefully have made a small but important contribution to that process.
Medical Students and Primary-care Residents
Nothing could be more satisfying in SETMA’s history and advancement than the opportunity to be entrusted with introducing senior medical students and primary-care residents to the practical applications of best practices, evidence-based medicine, informatics, analytics and PC-MH. As we complete this syllabus, July 29, 2013 rapidly approaches when the first senior medical student will arrive from the University of Texas Health Science Center at San Antonio School of Medicine for a four-week externship. In August, we expect our first family practice residents from the Texas A&M School of Medicine to participate in an externship as their two Chief Residents spend several weeks at SETMA.
This syllabus will evolve and our understanding of how we can improve students’ experience at SETMA will grow; but, our commitment to excellence in healthcare and our belief in our responsibility to contribute to the training of the next generation of nurse practitioners, physician assistants, physicians and other healthcare colleagues will remain constant.
The course objectives for SETMA’s Senior Medical Student Externship in Pateint-Centered Medical Home are to identify, describe and define:
- The critical role of primary care in healthcare transformation.
- Why the future of healthcare is dependent upon primary care.
- Why the only segment of medicine which can effect sustainable change is primary care.
- Why the best and the brightest will find the greatest fulfillment in primary care.
- How patient-centered medical home is the hub and the core of healthcare transformation.
- Show students how excellence in care and practice financial stability are not mutually exclusive.
This syllabus includes the following sections and content:
Section I - The History and Philosophy of SETMA
SETMA’s Mission Statement was enunciated in October, 1997, two years and two months after SETMA’s founding. It states:
“To build a multi-specialty clinic in Southeast Texas which is worthy of the trust of every patient who seeks our help with their health, and to promote excellence in healthcare delivery in by example.”
This section is a brief description of SETMA’s commitment to excellence in practice and education. It includes an outline of the entire syllabus which is the backbone of the on-line electronic version of the syllabus.
In that this externship is about Patent-Centered Medical Home, the display of SETMA’s accreditations and recognitions from NCQA, AAAHC, and the Texas Physician Practice Quality Improvement Award demonstrates SETMA’s commitment to both practicing excellent medicine and also to complying with published standards. These accreditations and recognitions give credibility to SETMA’s approach to PC-MH.
SETMA is often asked, “How have you accomplished this transformation?” In an attempt to answer this, we have begun the preparation of a “developmental history” of SETMA. More than a narrative or chronological telling of SETMA’s story, this is an attempt to help others know the dynamic of SETMA’s growth and development. It is a “how,” if you will, others can take the best of SETMA, plant it in their soil, and organically grow another unique organization.
There are almost 300 Models of Care published in the medical literature. Perhaps the best known is described as “The Chronic Care Model (CCM) (which) originated from a synthesis of scientific literature undertaken byThe MacColl Institute for Healthcare Innovation in the early 1990s. During a 9-month project funded by the Robert Wood Johnson Foundation (RWJF), an early version of the Model underwent extensive review by an advisory panel of experts and was then compared with the features of leading chronic illness management programs across the U.S. Subsequently, the Model was further refined and published in its current form in 1998. Improving Chronic Illness Care, a national program of RWJF, was launched in 1998 with the Chronic Care Model at its conceptual core.”
Most “models of care” owe a debt to the MacColl Institute’s work, as does SETMA. As this syllabus is prepared, SETMA is involved with an on-going research project with the RWJF and the MacColl Institute entitled: The Primary Care Team: Learning from Effective Ambulatory Practices (PCT-LEAP. (An introduction to that work can be reviewed at http://jameslhollymd.com/letters/Robert-Wood-Johnson-Foundation-PCT-LEAP.)
An explanation of and an experience with SETMA’s Model of Care will be central to the externship. The five parts to the Model are:
- Tracking one patient at a time the fulfillment of over 300 quality metrics. The concepts of “clusters” and “galaxies of quality metrics will be explained.
- Auditing by population or panels of patients provider performance on these metrics.
- Statistically analyzing provider performance and patient characteristics to find leverage points for improvement
- Public Reporting by Provider Name on SETMA’s website of provider performance. Few things have been as motivating as this for quality improvement.
- Quality Improvement Initiatives designed on the basis of the data and information from the first four steps of the Model.
Among SETMA’s most recent and novel innovations, The Automated Team involves the advancement of clinical decision support to the point of maximizing the use of electronics in quality care initiatives. The essential element of the Automated Team is that when a patient makes an appointment, the computer searches the patient’s entire data base and on the basis of the patient’s chronic illnesses, gender, age and risk profile determines what preventive care, screening care, state of health evaluations and standards of care are needed by the patient.
All procedures, tests, referrals, evaluations, points of care, etc., are then automatically initiated. Simultaneously, three documents are prepared prior to the patient’s visit: one for the nurse; one for the provider; and, the most important for the patient which lists for the patient all of the care which has been ordered prior to their visit. The documents also describe to the patient why the care is important and when and where it will be obtained. Including in the patient’s document will be an explanation of the nurse’s and the provider’s responsibilities. SETMA believes that this innovation has the potential for revolutionizing healthcare as it frees the nurse and provider from many tasks, leaving more time for personal interaction with the patient.
SECTION II - Electronic Medical Records (EMR) - Electronic Patient Management
This extensive document was prepared by SETMA in 1999 and was published in booklet. It allowed our patients to know where we were headed with electronic patient records and in retrospect, it laid the foundation for SETMA becoming a patient-centered medical home before we had ever heard the term. Many and most of the element of PC-MH are contained in this manuscript. Its review will help the student see how effective and excellent future advances and transformation will logically and necessarily be built upon past work and accomplishments.
SETMA cannot be understood without knowing the impact that Dr. Peter Senge’s The Fifth Discipline had upon SETMA’s development, upon the design of our Model of Care and upon the deployment of our EMR. The complexity of medical knowledge is created both by its volume and by the manner in which that information is packaged. Applying that complex knowledge-base effectively will require a fundamental shift in physician approach to information.
Electronic medical records (EMR) provides the means for that shift but does not necessarily dictate that such a shift will take place. Often, EMR is only used as a glorified transcription tool whereby a patient encounter is documented electronically, without providing significant advantages in processing of information, and without the patient’s care profiting from sound science.
Change is not easy. It often creates anxiety and insecurity, even, and maybe especially, among healthcare providers. However, to create excellence in healthcare, which is more of a process than it is a characteristic of a product, providers must continually be "learning" which will require a change in the understanding of the nature of learning and will also require the elimination of barriers to learning. To sustain the learning process created by this "shift of mind" healthcare providers need tools which facilitate change rather than processes which support the status quo. The externship will help the student, at whatever level of training, understand the sustainability of excellence through morphing from the pursuit of EMR to the pursuit of electronic patient management.
This document was prepared in 2006 and is entitled Beyond Electronic Medical Records: the Hope and Promise of Electronic Patient Management. Coupled with the 1999, “More Than a Transcription Service,” this document helps the student observe the continuing development of the philosophical and intellectual foundation of the PC-MH transformation, before the term was ever used.
If there is one thing which is needed in medical informatics, or medical information technology world, it is a “change of mind.” There needs to be a fundamental change of mind such that we are not talking about "electronic patient records (EMR)," but about "electronic patient management (EPM)."
Transitioning from an EMR mentality to an Electronic Patient Management (EPM) goal is to apply Dr. Senge's concept of "generative learning" to the field of medicine. Addressing the concept of a "learning organization," Senge said:
"This then is the basic meaning of a learning organization... continually expanding its capacity to create its future. For such an organization, it is not enough merely to survive. ‘Survival learning’ or what is more often termed ‘adaptive learning’ is important - indeed it is necessary. But for a learning organization, ‘adaptive learning’ must be joined by ‘generative learning,’ learning that enhances our capacity to create."
If we continue simply to talk about electronic patient records, we may create a future in which we discover that we have only created a very expensive and very complex substitute for a relatively inexpensive transcription service. If we are going to impact the future of health care, we -- vendors, managers, providers, payers, institutions, every member of the health care team -- are going to have to begin thinking differently. This will involve at least three major shifts in our thinking. This will involve “Medical metanoia.”
This part of the syllabus is intended to introduce the student to the necessity for ongoing development of the tools and innovations surrounding “systems thinking” in healthcare and particularly in healthcare informatics. Perhaps the two most difficult aspects of healthcare is the maintenance of accurate, up-to-date and complete medication lists and chronic problem lists. As an illustration to the systems approach to problem solving, this work will be reviewed with the student to show how imperative it is that the power of electronics is used to solve complex problems and to make it “easier to do a critical task well than not to do it at all.”
SECTION III - Population Management
This will introduce the student to the concept of the Triple Aim and its key role in healthcare transformation. The history, intend and content of the Triple Aim will be discussed and how a robust EMR deployment can help fulfill the Triple Aim will be described.
Population management requires data analytics in order to discover leverage points for care improvement. This will introduce the student, not so much to the science of analytics, but to the application of statistical methods to quality care improvement.
Whether in the PC-MH or in the traditional healthcare environment, ultimately all problems and all solutions start with Transitions of Care. This study will introduce the student to SETMA’s 14 key developments which allow effective care transitions to take place and showing its impact on preventable readmissions, patient safety and patient satisfaction with care.
Introducing the student to quality audits and to quality metrics (principles, philosophy and impact on care) is key to PC-MH. This review will familiarize the student with the vocabulary and the practical applications of quality auditing in relationship to Transitions of Care. The impact of documenting the patient’s care in the same data base at all points of care will be illustrated, also.
Major efforts are being made to pay primary care providers for the unique work they do. CMS’ publication in January, 2013 of new ICD-9 and new CPT codes for Transitions of Care Management payment is illustrative of that effort. This study will allow students to see the connection between excellence of care and reimbursement strategies.
SECTION IV - Disease Management Tools
This section will introduce the student to disease management tools developed by SETMA to standardize the care and to improve the care of multiple, common, chronic conditions. In May, 1999, SETMA realized that EMR was an inadequate goal for healthcare informatics and that SETMA wanted to leverage the power of electronics to improve the care of individual patients and of groups or populations of patients. In 1999-2000, SETMA developed a diabetes disease management tool. In retrospect, we discovered that the deployment and use of this tool alone resulted in an improvement in the mean hemoglobin A1c of .36%. Over the next several years the development of an American Diabetes Association Diabetes Self-Management Education program had a similar impact and finally the addition of an endocrinologist had a lesser but a significant impact on that measure.
It was the development of the diabetes disease management tool which set SETMA on course to becoming a Joslin Diabetes Affiliate in 2010 after a 2003 presentation of SETMA’s Diabetes Management tool to Joslin in Boston. As will be seen under the “preventive medicine” section, primary care excellence of care of diabetes should always include a diabetes prevention program.
Disease Management tools not only standardized the care SETMA gives to all patients, it also allowed the development of individualized Plans of Care and Treatment Plans which is a significant requirement of PC-MH recognition. SETMA’s ability to provide these education and treatment tools to patients was enhanced by the placement of laser printers in all examination rooms. This was expensive, but increased efficiency and excellence and illustrates for the student how the use of technology can expedite excellent care.
This tool illustrates for the student how it is possible for a practice to develop auditing tools when none are published by national agencies. While lipids are a critical part of primary care practice, particularly in risk stratification and in cardiovascular risk mitigation, no national, standardize quality metric set exists. Therefore, SETMA created its own. guided by evidence-based medicine. PC-MH recognition requires a practice or provider to focus on three important disease states. Over 95 percent of practices initially focused on diabetes, lipids and hypertension. At least for NCQA, the 2011 Standards required one of those three important conditions to be a behavior care issue.
SETMA’s focus on high blood pressure management reflects its prevalence in our practice - 55% of our adult patients have a diagnosis of hypertension - and its value in risk reduction. Well accepted, but sometimes not a conscious aspect of care, is the reality that the cardiovascular risk reduction for patients with diabetes is more benefited by blood pressure control than by blood glucose control. All of SETMA’s disease management tutorials are more than a “how to use our computer” and are true “disease monument tools” focusing on evidence-based medicine. With SETMA’s disease tutorials, it is possible continuously to refresh the student’s or providers’ knowledge of best practices.
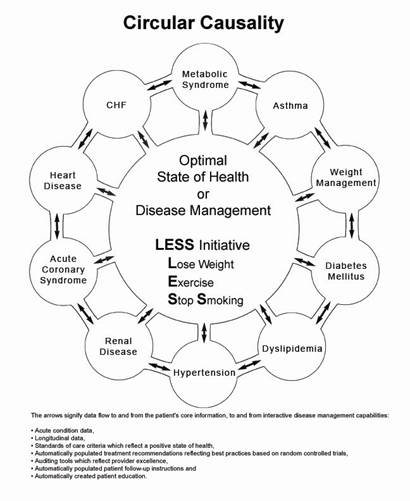
No doubt the most interesting and maybe controversial disease process is the Cardiometabolic Risk Syndrome. SETMA’s tool incorporates the best knowledge and evidence for the improvement of this fascinating and complex entity. The interaction of multiple disease processes makes Cardiometabolic Risk Syndrome a perfect tool for learning how integrated a patient’s care must be in order to achieve maximum health benefit. Through this study, the student will be introduced to the concept of “circular causality” in disease management which is illustrated by the following:
In 2006, the American Medical Association published an Adult Weight Management Treatment Program. This 220-page notebook included excellent material. The AMA sent the first 30 copies of this program to SETMA. Finding it excellent but impractical to use, SETMA reduced the program to an electronic format which made it accessible to be used in daily clinical practice. The student will be exposed to how to take excellent resources and to adapt them through electronics to daily practice. This program is a part of SETMA’s LESS Initiative which has been published by the Agency for Healthcare Research and Quality on their Innovation Exchange.
SECTION V - Preventive Management Tools
Every primary care provider wishes to help patients improve their health. Modification of behavior is a part of this improvement, particularly in three areas: losing weight, exercising and stopping smoking. Doing this with a single patient is easy but how about 700 patients a day? The LESS Initiative (Lose Weight, Exercise and Stop Smoking) is SETMA’s major preventive care and behavior modification tool. This study will illustrate for the student: how to systematize complex care opportunities; how to audit them; and, how to improve performance on them.
Evidence-based literature affirms that if a patient is given a written, personalized exercise prescription and if the provider addresses this issue at each visit, the patient is more likely to sustain a personal exercise program. Employing the Cooper Aerobic study results, SETMA provides each patient with their own exercise plan; illustrating to the student how to take a complex problem and to making it easier to it right than not to do it at all.
Excellence in the treatment of diabetes includes the prevention of diabetes, as the best way to treat diabetes is still, “don’t get it,” when that is possible. Using algorithms for screening and with auditing of appropriate follow-up, along with providing the patient with education materials showing the “progression to diabetes,” SETMA aggressively alerts patients to their risk of developing diabetes which is a part of The LESS Initiative and engages patients in how to avoid diabetes.
Ninety percent of patients fifty-five years of age, who do not have hypertension, will develop hypertension it in their lifetime, if steps are not taken to avoid it. This knowledge and the knowledge of the cardiovascular, cerebrovascular and peripheral vascular dangers of hypertension drive SETMA to focus on its prevention. The student will learn how to risk stratify patients and how to personalize care based on that risk.
SECTION VI - Risk Stratification
How many tasks can you ask a provider to complete at each encounter and also expect them to do them consistently? The answer requires answering three other questions. They are:
- "How important is the task"
- "How much time does the task take"
- "How much energy does the task take?"
If the task is very important it might be done, but if it requires more or excessive time or energy, it will likely not be done." It is possible to ask providers to do 30 or 40 things at each patient encounter, if those things are very important, takes little or no time and takes little or no energy. We ask that or more of SETMA providers.
The following will illustrate for the student this principle. In August of 2010, the American Board of Family Medicine (with which SETMA is currently involved in a research project) published an article recommending that every five years Family physicians calculate one Framingham Risk Score for each of their patients. For years, SETMA has calculated multiple Framingham Scores at each encounter.
About the same time this 2010 article was published, SETMA launched the calculation of all 12 risk scores but we added a complexity. We added a "What If Scenario" to each calculation. The "What If Scenario" was suggested by the application of one of IBM's 'Change Agent Principles" which states, "If you are going to make a change, it had better make a difference!" The idea is that if we are going to ask patients to change behaviors or habits, that change had better make a difference and to complicate the proposition, the change we are asking them to make, will not show a difference for thirty or forty years.
With the calculation of all 12 Risk scores and with the "What If Scenarios," we can quantify the potential difference or impact the change we are asking the patient to make. For instance, if the patient’s actual heart age is 50 years, but the Framingham Risk Score calculates that their relative heart age is 73 years, the "What If Scenario" shows the improvement in the relative heart age if all elements employed in that calculation:
- Are treated to goal
- Are treated to a 20% improvement
- If One element such as blood pressure is treated to goal
- If another element such as lipids are treated to goal
- If another element is treated to goal such as diabetes
The Hierarchical Condition Categories (HCC) are a risk stratification device created by the Centers for Medicare and Medicaid Services (CMS) to allow the rewarding of providers and organizations which assume responsibility for caring for patients who have complex, multiple chronic disease. Because the HCC scores are important in Medicare Advantage, Medical Home and Accountable Care Organizations the student will be introduced to this concept. This again is a means of showing the relationship between excellent care and excellent primary care reimbursement for the care delivered. This part of the syllabus also introduces the student to the potential correlations between HCC Code Coefficient Aggregates and E&M Coding:
SECTION VII - Unique Functions
How does a provider remember to follow-up with a patient about an important test result or need for additional testing or services? This tool introduces the student to a reminder system.
You see a patient who is not fasting but their care requires fasting labs. How do you efficiently get them to return to the clinic on a given day to have their labs ordered? The Future Lab Function will show the student how complex but simply problems can be solved electronically.
Texas providers have 78 conditions for which they are responsible for reporting. How do you take that complex task and make it simple requiring no time and no energy on the part of the provider?
It is easy to tell if a patient is dehydrated currently. But how do you document that a patient was hydrated when you saw them six weeks ago, when the patient is dehydrated today? This electronic tool shows one solution.
Hospital Consumer Assessment of Healthcare Providers and Systems surveys are a critical part of assessing whether the care patients are receiving is patient-centered. SETMA has designed a solution for:
- Letting providers know what they are responsible for in patient satisfaction surveys.
- Letting providers know how they are performing in patient satisfaction surveys, daily.
- Letting providers know how to improve their performance on these surveys.
This is a critical part of patient-centered care.
This syllabus will be presented to our first student, Ms Summer M Scavone, upon her arrival on Monday, July 29, 2013. She will also receive a schedule for her four weeks with SETMA. It is our hope to make a positive contribution to her professional career.
|