|
Using SETMA’s Disease Management tools Diabetes, Hypertension and Lipids to fulfill the NCQA requirements for a written Plan of Care and Treatment Plan
Providing our patients a written personal Treatment Plan and a written personal Plan of Care for diabetes, hypertension and lipid management are requirements for achieving Tier 3 recognition by NCQA as a Patient- Centered Medical Home. For over seven years, SETMA has been producing Follow-up Documents for each of the chronic diseases on which we are now reporting in our becoming a Medical Home.
We have made modifications in these tools so that the Follow-up Document fulfills all of the requirements for a Treatment Plan and a Plan of Care. (This tutorial addresses only the Treatment Plan and Plan of Care. For a full review of the disease management tools see the tutorial on each.)
Assessing the Cardiovascular Risk Score of Each Patient
In order for the Treatment Plan and the Plan of Care to be precise and specific for each patient, it is important that you first complete the Framingham Cardiovascular and Cerebrovascular Risk Scores and the Global Cardiovascular Risk Score before using the below functions.
(Note: You only have to complete the risk scores once on each visit, after which the score is displayed on all of the disease management tools and will work interactively with the Treatment Plan and Plan of Care.)
In completing the Risk Scores, you will also be fulfilling another of the NCQA Medical Home Requirements which is the assessment of the risk of future disease for patients.
Using the Framingham Cardiovascular Risk Score
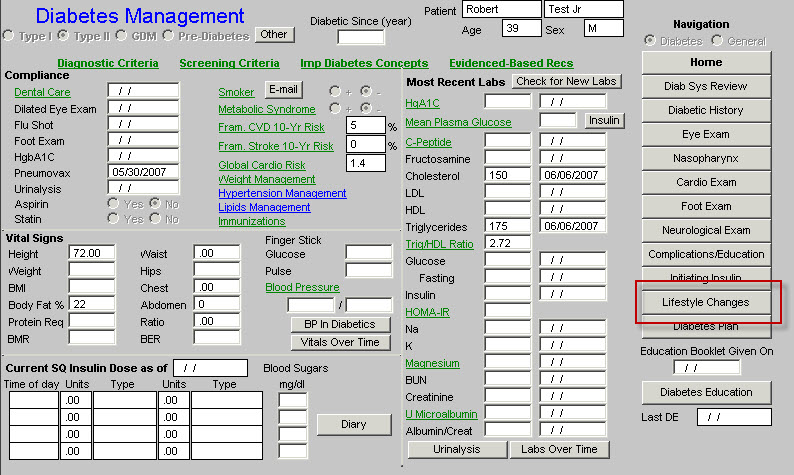
You can find the Framingham Risk Scores calculation tools on each of the Diabetes, Hypertension and Lipid Disease Management tools. The following illustrates its location on the Diabetes Template.
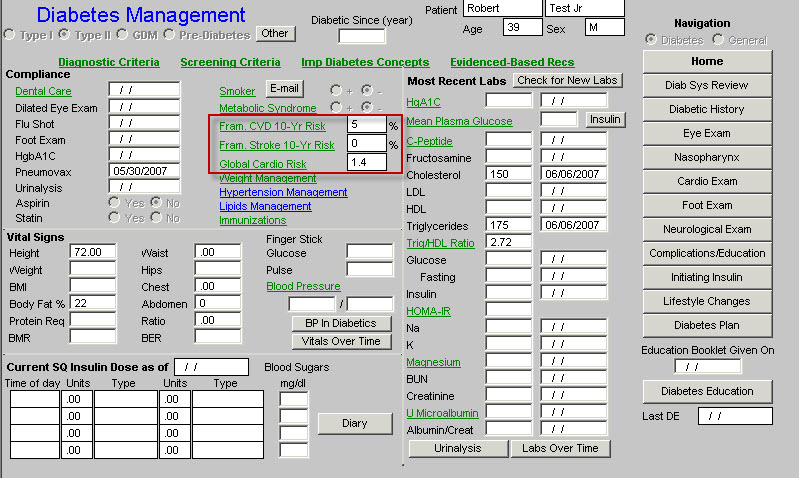
On any one of these templates activate the button entitled Fram CVD 10- year risk
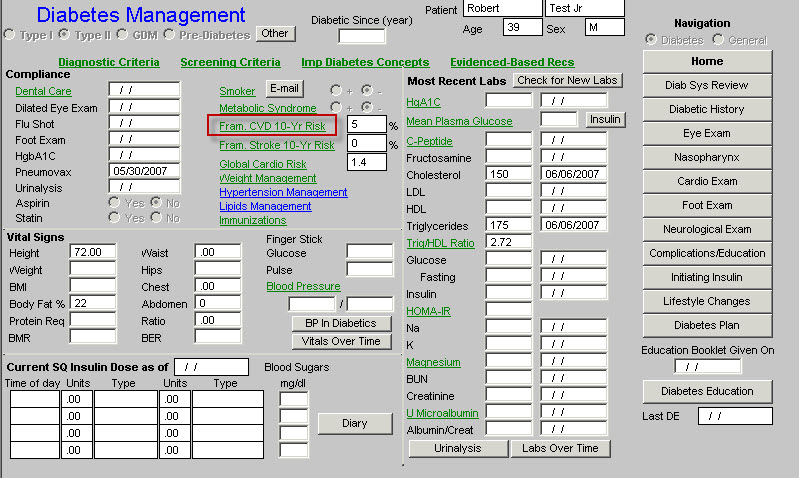
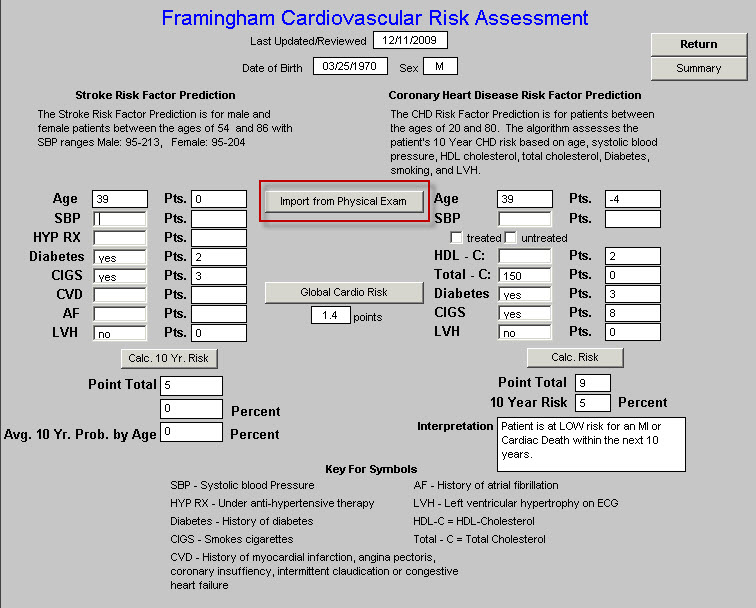
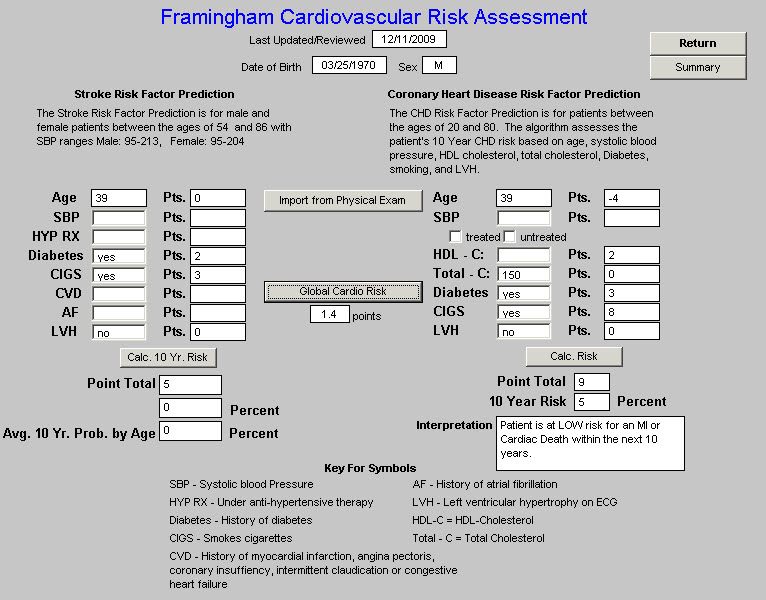
This launches the following template. To complete the Fram CVD 10-year risk activate the button entitled Import from Physical Exam
Complete the check box which indicates whether the patient’s blood pressure is treated or not, i.e., is the patient on blood pressure medication.
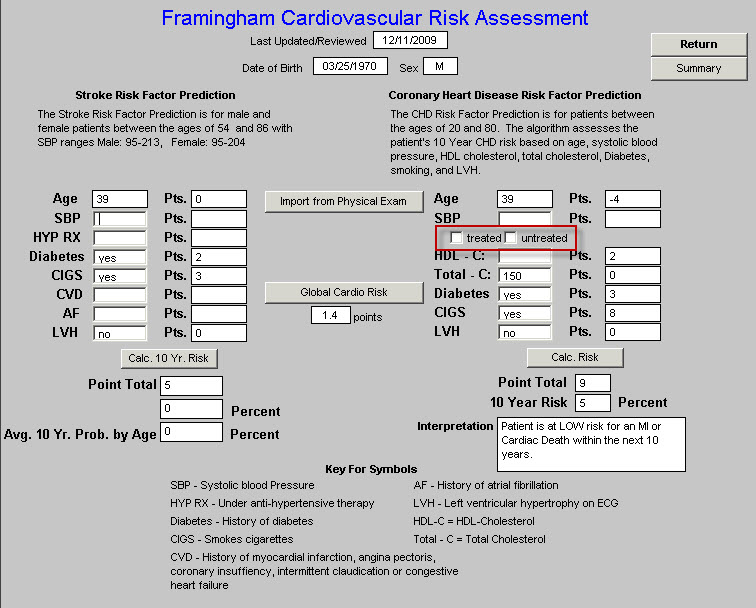
Click the button entitled Calc Risk
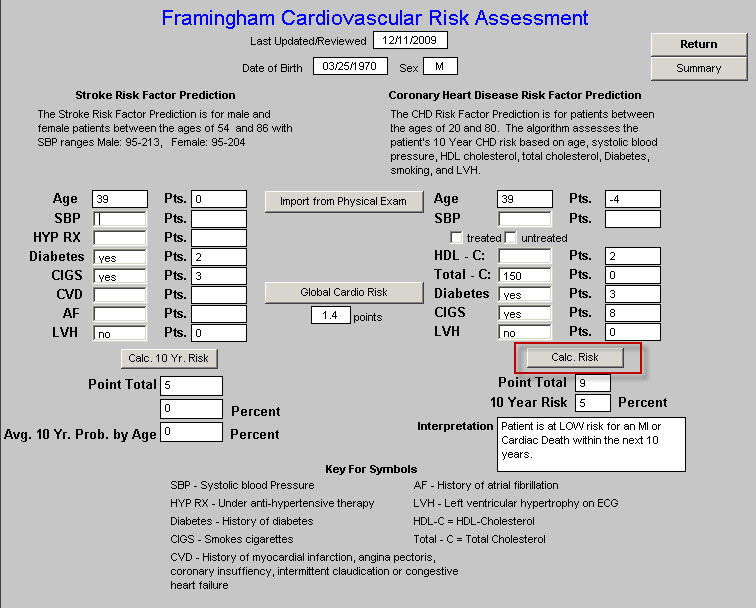
The Risk Score will now be displayed on this template, on each of the disease management tools and it will also be used in preparing your Treatment Plan and your Plan of Care for each patient.
Using the Global Cardiovascular Risk Score
Several years ago, it was recognized that the Framingham Score weightedthe patient’s age so heavily that some young people with high cardiovascular risk were missed and some older patients with lower cardiovascular risk were misjudged as being at high risk.
An analysis was done of the Framingham Data and the Global Cardiovascular Risk Score was created. This score uses the Framingham Data but eliminates the age and gender bias, adding Hemoglobin A1C to the assessment. If the score is above 4, the patient is considered to have high Cardiovascular Risk.
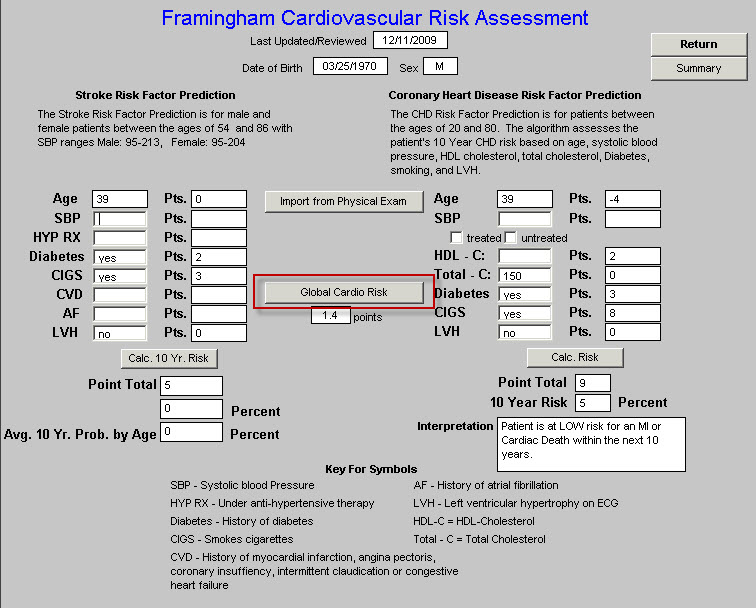
To use the Global Cardiovascular Risk Score click the button in the middle of the Framingham Cardiovascular Risk Assessment template entitled Global Cardio Risk.
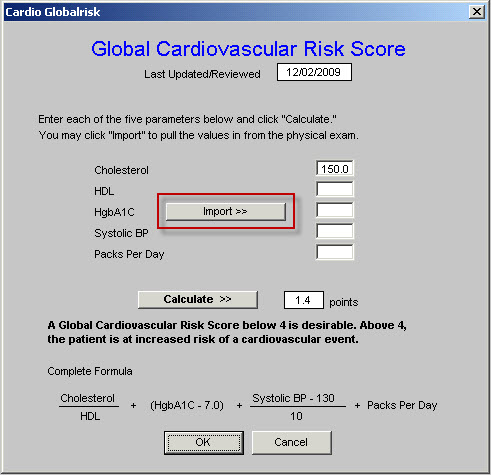
This launches the following pop-up. Activate the button entitled Import. This will aggregate the data required to calculate the score.
To complete this process, activate the button entitled Calculate
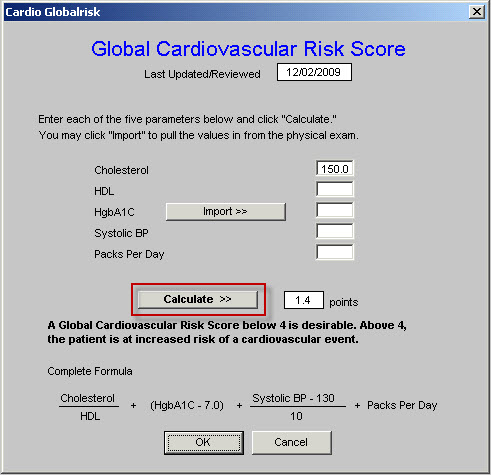
The score will be displayed on this screen, on all of the disease management tools and will be used in preparing your Plan of Care and Treatment Plan on each patient. A value above 4 indicates that the patient is at increased risk.
The principle difference which you will find is that at times young people who have a low Framingham risk score, will have a high Global Cardiovascular risk score and older people who have a high Framingham Score will have a lower Global cardiovascular risk score. This is because of the elimination of the age as a factor.
To return to the Framingham Cardiovascular Risk Assessment template click OK
Framingham Cerebrovascular Risk Score
Completing the Framingham Cerebrovascular Risk Assessment is done as follows. In the Stroke Risk Factor Prediction column to the left of the screen complete any items which are not displayed.
If any of the items are unknown to you, leave them blank. If on the GP Master History template, under Cardiovascular History, you have denoted that the patient has LVH, that will be auto filled on this template.
Once you have filled in all of the items, depress the button entitled Calc 10 Year Risk
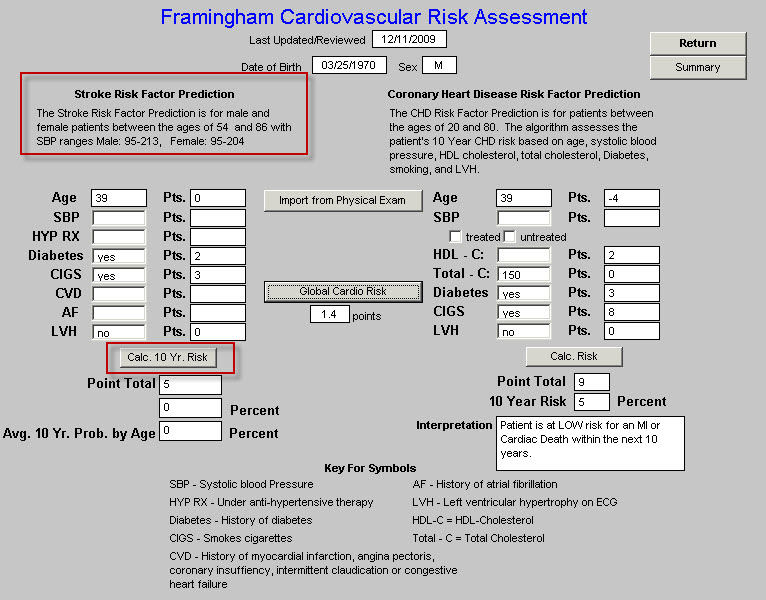
You are done.
The Cerebrovascular Risk Score will be displayed on all disease management tools and will be used in calculating your Treatment Plan and Plan of Care. While it takes longer to review this tutorial and to learn how to use this function, it only takes a few seconds to complete it during a visit.
Using SETMA’s Disease Management tools Diabetes, Hypertension and Lipids to fulfill the NCQA requirements for a written Plan of Care and Treatment Plan
Definitions:
- Treatment Plan: “A written plan detailing the medical regimen as ordered by the physician, including periodic monitoring for adverse reactions and other follow-up care.”
- Plan of Care: “a written plan for services that will be provided to the patient to meet their identified needs.”
Diabetes Treatment Plan and Plan of Care
You will find the Diabetes Disease management Tool by going to AAA Home
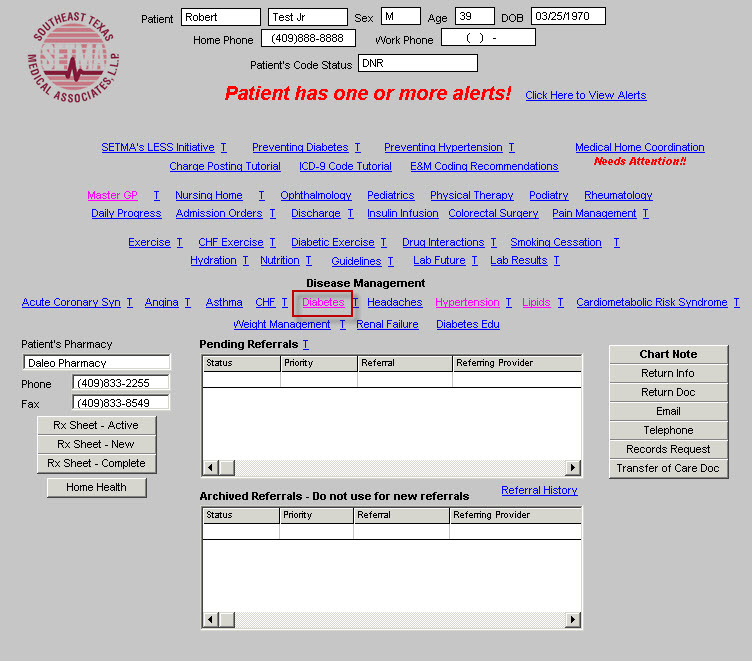
Click on the button entitled Diabetes and the Diabetes Disease Management tool is launched.
All of the evaluation and documentation which you have done on GP Master will populate this tool as well. While this tool can be used as a complete guide to the treatment of diabetes, it may also be used for our current purpose.
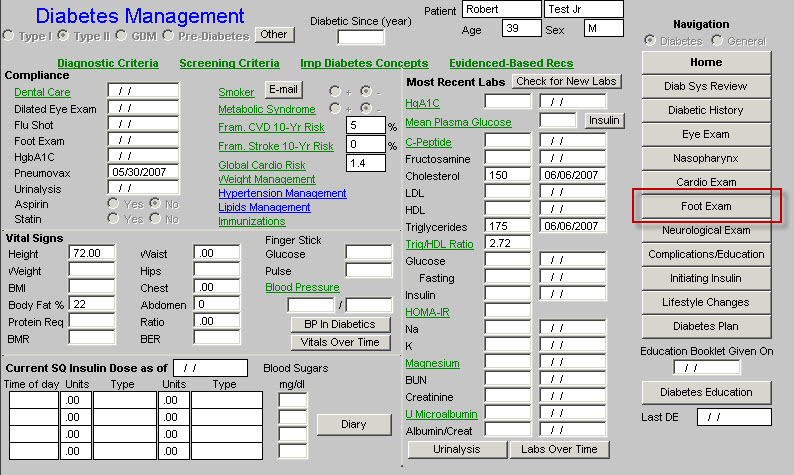
To use the tool for Treatment Plan and Plan of Care, make certain that the “10 Gm Monofilament foot examination” has been done. You will find that examination by clicking on “Foot Exam” above
From the Diabetes Management template, click on the navigation button entitled Lifestyle Changes.
You will then see the following template
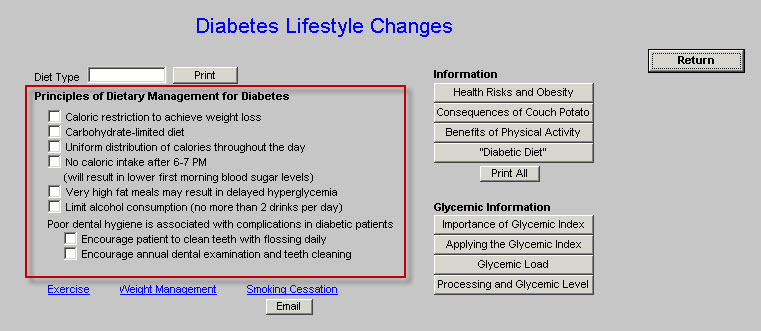
This template automatically selects the Principles of Dietary Management for Diabetes. Click on Return.
This returns you to the Diabetes Management template.
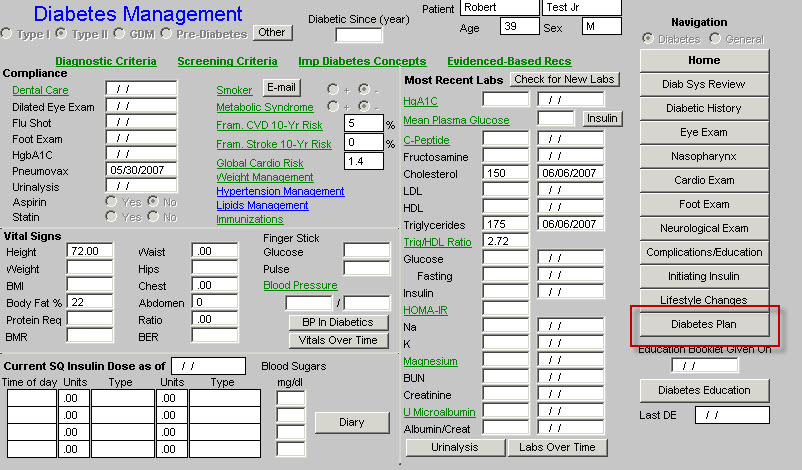
Now, click on Diabetes Plan. This launches the Diabetes Plan template.
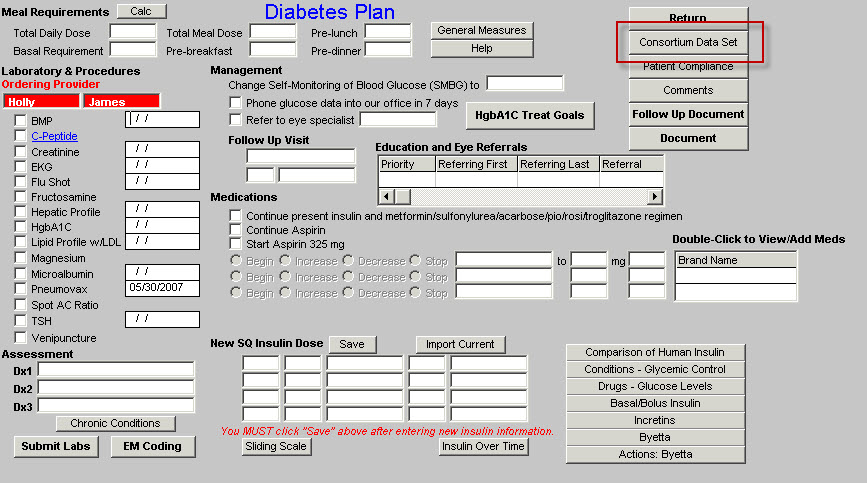
You may review the Consortium Data Set from this template or from the Medical Home Coordination Review template. Once you review the Consortium Data Set to make sure that your comprehensive diabetes measures have been met, click on Follow-up Document
This creates the Follow-up document which has all of the elements of a written Treatment Plan and a written Plan of Care.
- Print this document and give it to the patient. (You should review one of these documents so that you can tell your patient what this document contains and what you want them to do with it.)
- Make sure they receive the Follow-up Document before they leave the clinic.
- If you do significant modifications to the Treatment Plan and/or Plan of Care after reviewing the patent’s lab work, re-create the Follow-up Document and have it mailed to the patient.
You are through.
You have produced a document which is educational to the patient and which meets a standard of care of which you can be proud.
Lipid Treatment Plan and Plan of Care
You will find the Lipid Diabetes Disease management Tool by going to AAA Home
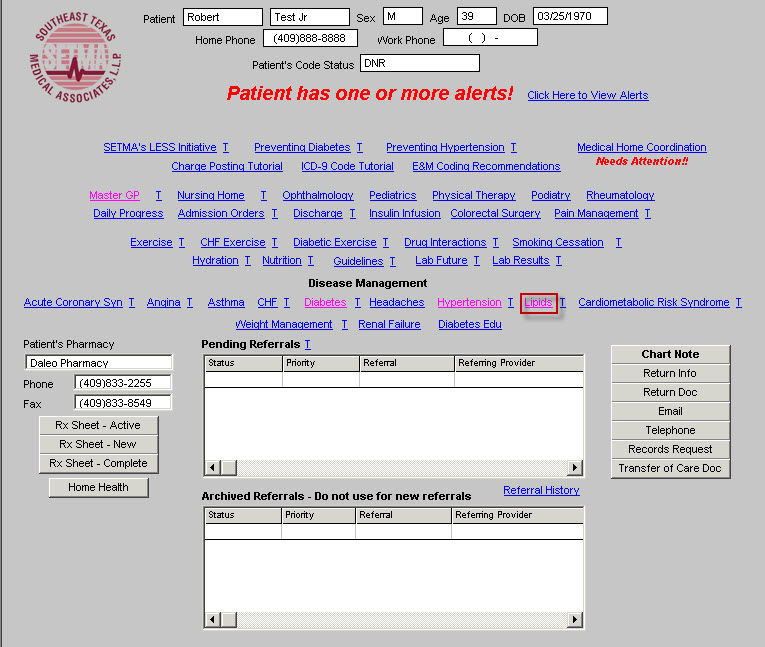
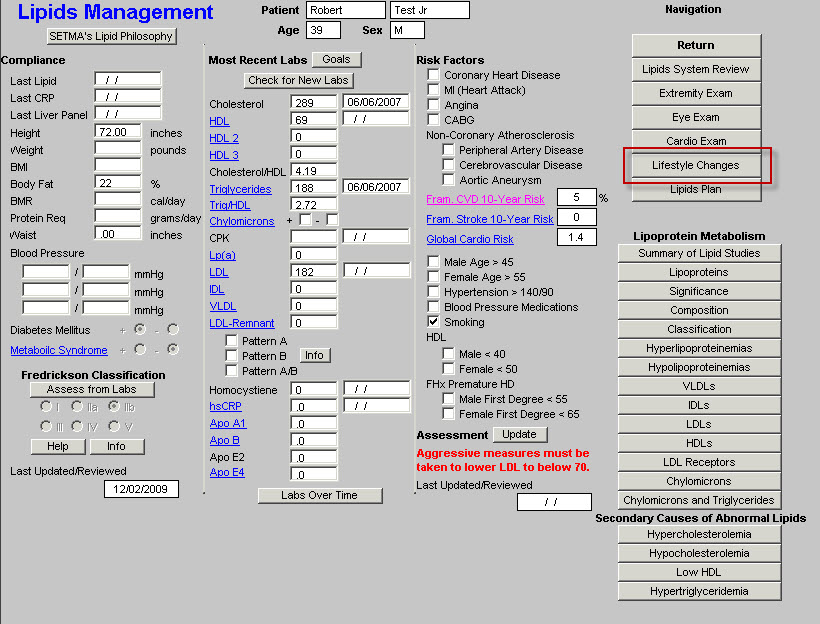
Click on the button entitled Lipids and the Lipids Disease Management tool is launched.
All of the evaluation and documentation which you have done on GP Master will populate this tool. While this tool can be used as a complete guide to the treatment of lipids, it may also be used for our current purpose.
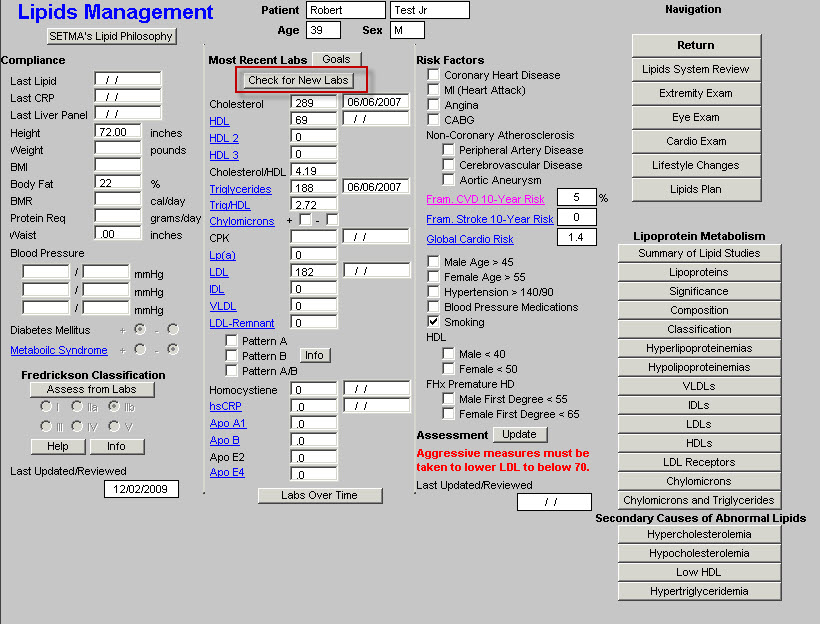
In order to make use the Fredrickson Classification function, click on the Check for New Labs button.
To use the tool for Treatment Plan and Plan of Care, click on Assess from Labs button at the lower left hand corner of the template.
If the patient’s lipid pattern matches one of the phenotypes in the Fredrickson Classification, it will be automatically denoted and an education document on that type will be added to the patient’s Lipid Follow-up Document. This will be done automatically.
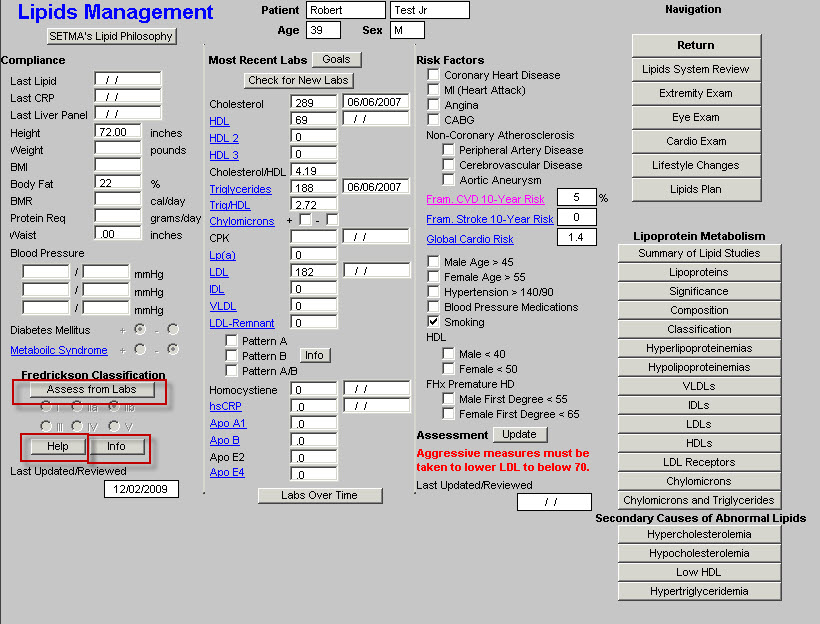
If you want to review this patient’s specific lipid-phenotype document, click on the button entitled Info at the bottom left of the template. If no type is automatically selected but you wish to assign one, just check the appropriate box.
If you wish to review the six phenotypes in the Frederickson Classification click on the button entitled Help also at the bottom left of the template.
Next click on the navigation button entitled Lifestyle Changes.
On the Lifestyle template, check the box by any of the diets which apply to your patient. You can click as many as apply. All of the diets which are checked will appear on your Lipid Follow-up Note.
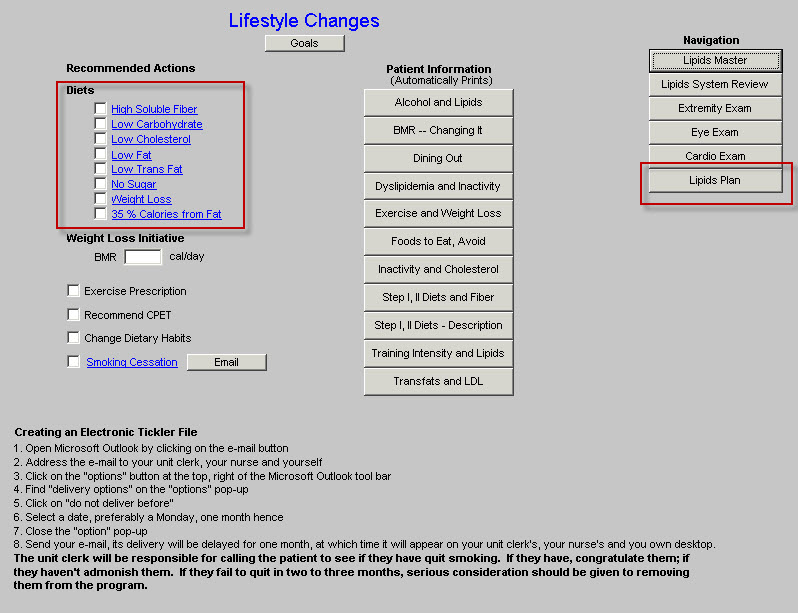
Click on the Lipid Plan navigation button. (see above Lipid Plan button in red)
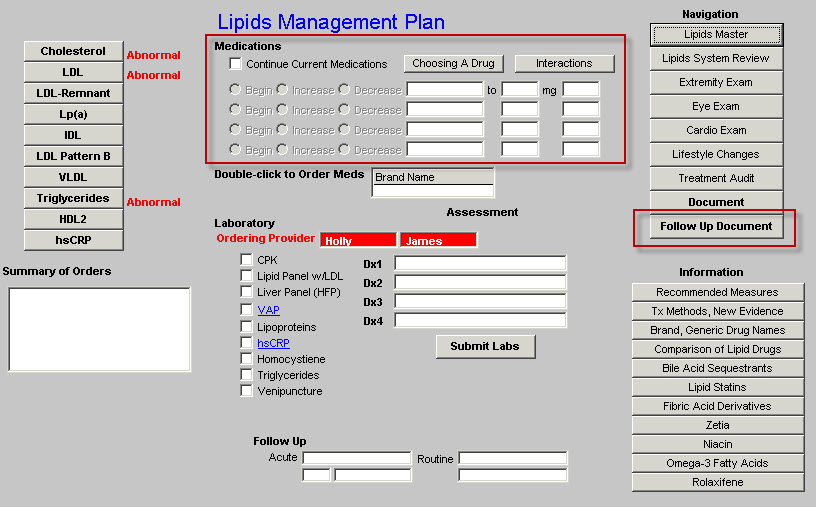
Note any changes in medications or note to “continue current medications”. Then click on the Follow-up Document. Print this document and give it to your patient.
You are done.
Hypertension Treatment Plan and Plan of Care
You will find the Hypertension Disease management Tool by going to AAA Home
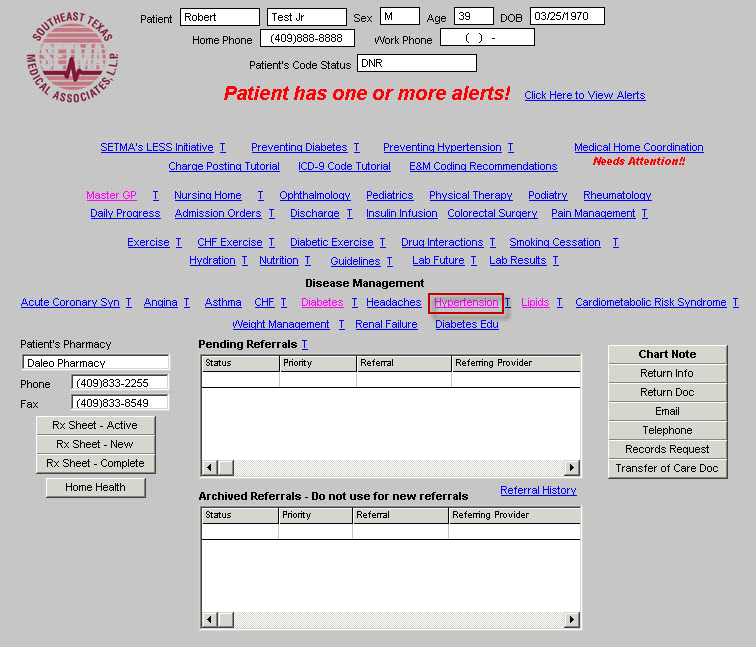
Click on the button entitled Hypertension and the Hypertension Disease Management tool is launched.
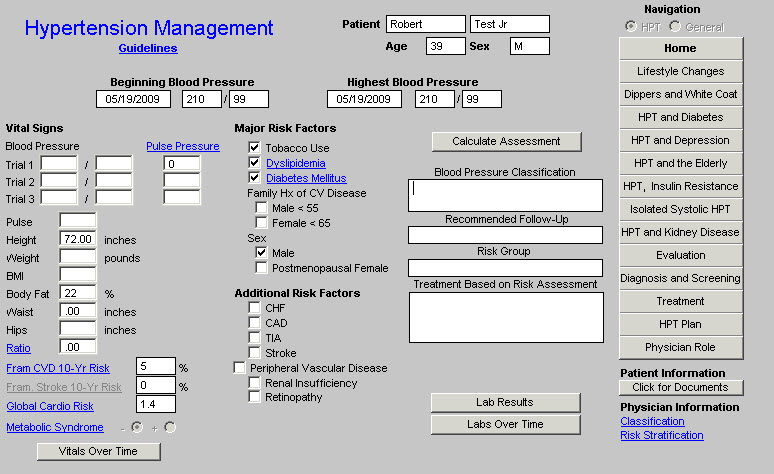
All of the evaluation and documentation which you have done on GP Master will populate this tool as well. While this tool can be used as a complete guide to the treatment of hypertension, it may also be used for our current purpose.
In order for this to fulfill all of the NCQA requirements for hypertension, you must click the button entitled Calculate Assessment
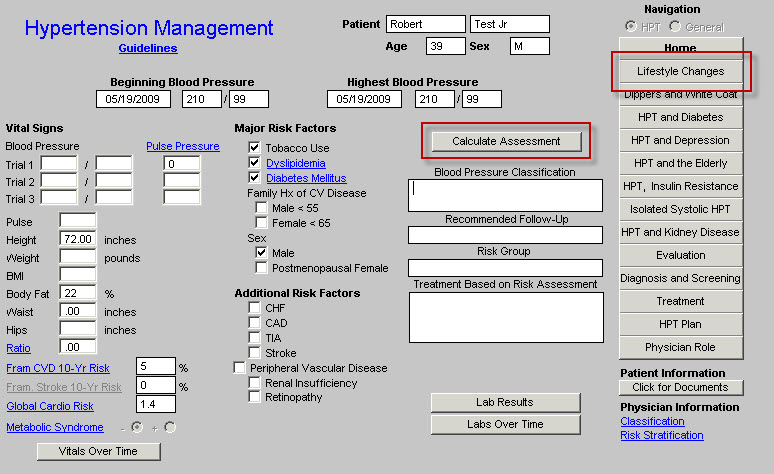
This displays the:
- Blood Pressure Classification,
- Risk Group,
- Recommendation and Treatment Plan based on the Risk Group. All of these are elements of quality measures for hypertension.
Now, in order to use the tool for Treatment Plan and Plan of Care, click on the navigation button entitled Lifestyle Changes.
This will display a template which addresses the major lifestyle changes which will significantly influence blood pressure, along with the potential reduction in systolic pressure which can be achieved by each. All of these will be automatically selected and they will also appear on your Treatment Plan and Plan of Care for hypertension.
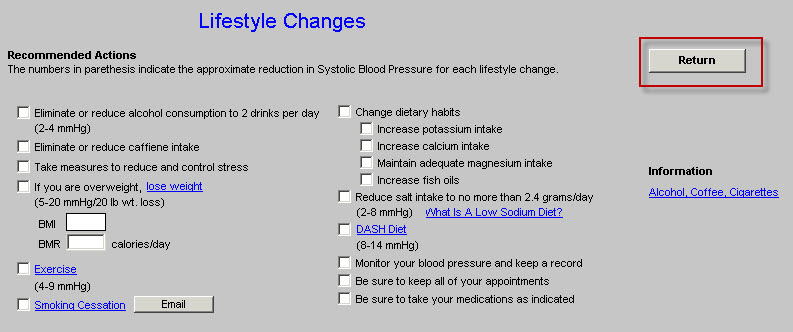
You ought to review the information on this template. There is also the ability for documenting Exercise and Smoking Cessation on this template.
Click on Return, which will display the Hypertension Master template.
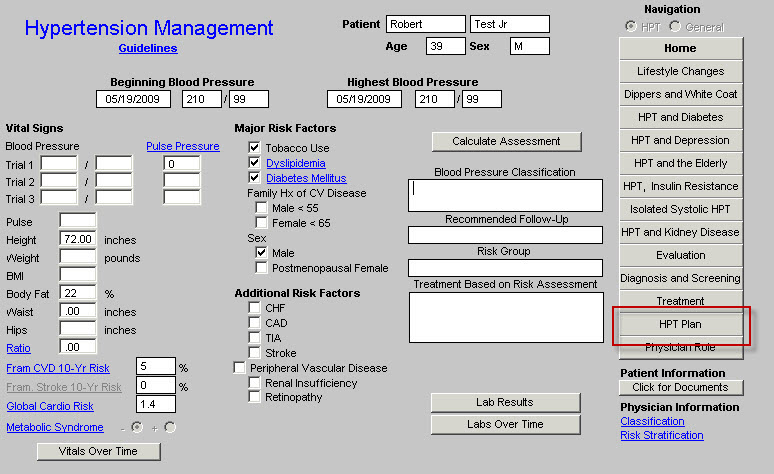
Now click on the button entitled HPT Plan
You need to do three things on this template:
- Complete the section on whether to “continue current medication” or “add or change a medication”
- Then click on the button entitled Follow-up Note.
- Then click on Return.
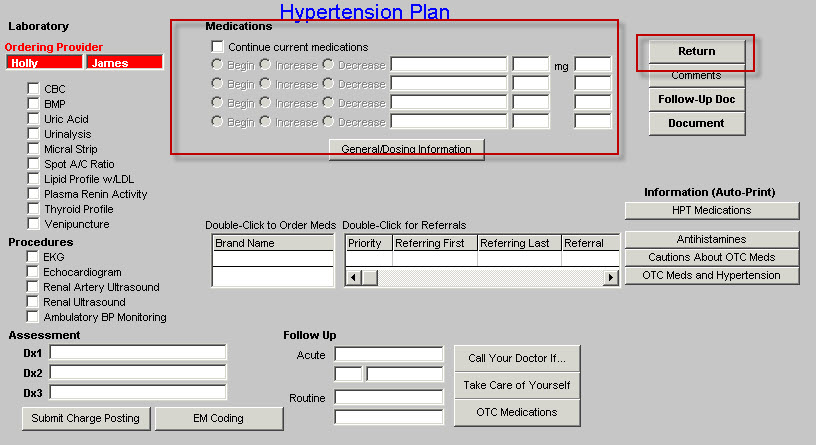
When you click on the Follow-up note, this creates note which you should give to the patient. It will also have material on the DASH diet and a low sodium diet.
This note will fulfill all of the requirements for a written Template Plan and for a written Plan of Care.
When you click Return, it will take you back to the Hypertension Master template.
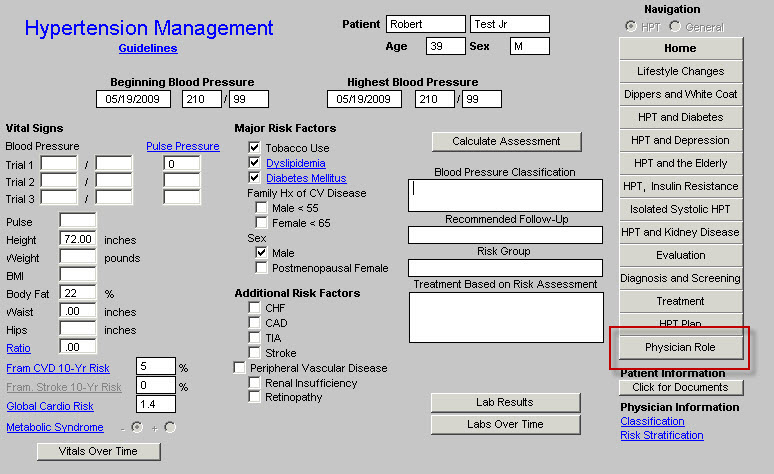
You may assess whether you have completed all of the appropriate measures for hypertension by clicking on the navigation button at the right of the template entitled Physician Role.
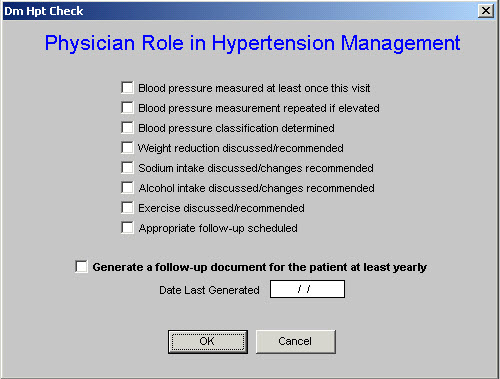
This same material can be reviewed from the Medical Home Coordination Review Template. Once you have reviewed this template, click OK.
You are done.
To use these three disease management tools to create robust, personalized, specific and complete Treatment Plans and Plans of Care not only meets NCQA requirements, but improves the quality of care which you will be giving to the members of your Medical Home.
Even if your patient has diabetes, hypertension and dyslipidemia, as many of our patients do, it takes only a couple of minutes to complete these tasks and to produce the documents which fulfill one of the most complex NCQA requirements. Once you give these documents to your patient, instruct them to read them and at their next visit review anything they do not understand, you have taken another step toward excellence.
| 