|
Patient-Centeredness
The power of patient-centered medical home is in putting the patient back into the center of the heath care process both in the care which is received and in the dynamic and operation of the medical practice. Patient-centeredness is reflected in the patient’s participation in the healthcare plan through a process which is called shared-decision making and through the manner in which healthcare providers relate to patients through a process called “patient-centered conversations”.
The measure of patient centeredness is done through two processes:
- In the inpatient setting, patient-centeredness is measured via the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS). This process is carried out by the hospital employing a vendor who samples inpatient care and reports HCAHPS scores to the hospital. SETMA has a process of its own for HCAPHS measurement. While this is not an officially endorsed process, it gives SETMA providers the opportunity to measure their own fulfillment of the HCAHPS scores. The following link explains SETMA’s process of fulfilling HCAHPS.:Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS): Tutorial for SETMA€™s Internal HCAHPS Survey
- In the outpatient setting, patient-centeredness is measured via the Consumer Assessment of Healthcare Providers and Systems (CAHPS). Like the HCAHPS in-patient audit, the outpatient CAHPS survey must be done by an independent vendor. From a list of vendors accredited by the National Committee for Quality Assurance (NCQA), SETMA chose the Myers Group ( http://www.themyersgroup.net) which will do quarterly auditing. We began this process in the fall of 2013.
Referrals
The process of shared-decision making takes place at several patient/provider interfaces, among the most significant of those is the referral process. The process of one provider sending a patient to another provider, or to another facility for care is a complex process which involves:
- Provider involvement of the patient in the decision making.
- Provider explanation to the patient of why the referral is required and what is to be gained.
- Provider determination as to whether the patient can meet the cost requirement of the referral.
- Provider making certain that the patient can carry out the requirements of the referral as to transportation, etc.
- Patient comprehending and concurring with the referral both as to content and the provider to whom he/she is being referred.
The larger a practice the more complex the referral process becomes. Some of those complexities are resolved at SETMA simply because the referral process is initiated at the point of service, making it possible to:
- Involve the patient in a shared-decision process about the need for a referral, to whom that referral will be made, the reason for the referral, and the timing of the referral
- The details of the referral require the above to be done before the referral can be completed.
- Track referrals, archive referrals and document when the response to the referral has been received and when that response has been sent to the provider.
- Document that the provider has received and has responded to the referral if required.
- In addition, the connection between referrals and the care coordination department is such that when a patient has three or more referrals initiated in a single day, an e-mail is automatically sent to care coordination which works to make the completion of those referrals as convenient as possible.
- Convenience for the patient which
- Results in increased patient satisfaction which contributes to
- The patient having confidence that the healthcare provider cares personally about him/her, which
- Increases the trust the patient has in the provider, all of which,
- Increases compliance in obtaining healthcare services recommended which,
- Promotes cost savings in travel, time and expense of care which
- Results in increased patient safety and quality of care.
(This analysis was first published by SETMA in August, 2011 at: Medical Home Series Two: Part VII Care Coordination. At the HIMSS Leaders & Innovators Conference at Amelia Island in November, 2011, Mr. Mark Bertolini, Chairman, CEO & President of AETNA used the phrase, “Convenience is the new word for quality."
“Convenience Is The New Word For Quality”
Initially, SETMA did not think that patient convenience was of sufficient value as to make it important to spend time and effort to increase the convenience of the care delivered. After developing the seven-step analysis above, and connecting the steps between convenience and quality, we realized that convenience really did contribute to and in reality result in quality care. In February, 2012, SETMA’s CEO gave a presentation to the HIMSS Leaders and Innovators breakfast that explained this concept. This is the link to that presentation: HIMSS 2012: Leaders and Innovators Breakfast Meeting
It is in this context that SETMA designed, deployed and uses our Referral template to fulfill the patient-centric element of this complex and critical element of medical practice.
Referral Tutorial
The referral template can be accessed from multiple sites in SETMA’s EMR application including:
- AAA Home
- Disease Management Tools Plan Templates (Diabetes, HTN and CHF)
- Plan Template
- Others
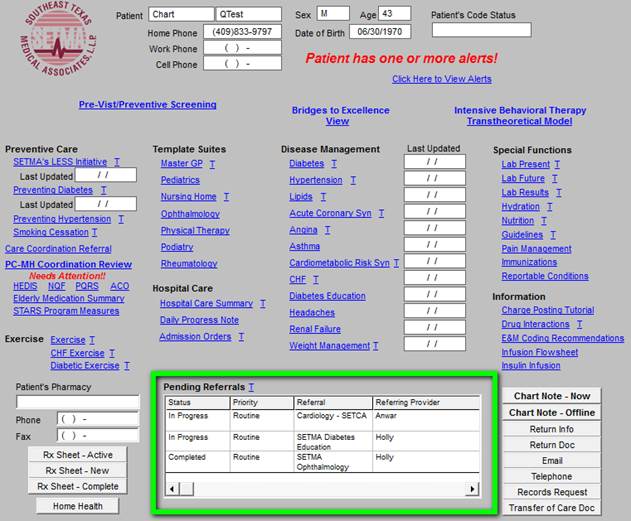
The following is the AAA Home Template; outlined in green is the referral function:
Note: When the "Referral Template" is accessed, the following fields are automatically completed: date, time, referring provider and status of referral. If after completing one referral, a second referral is initiated by clicking on the "clear to add" button, the "Auto fill" button must be launched in order to complete those fields.
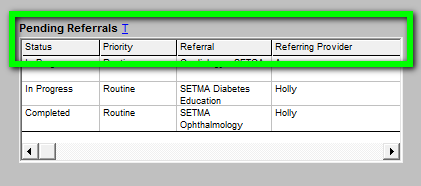
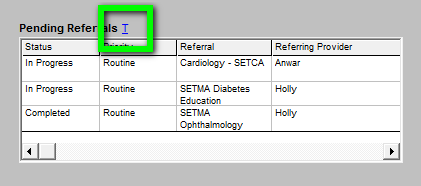
The referral template denotes the following elements of the referral process:
- Status: either “Pending” which means the referral has been initiated but not completed;
“Completed” which means that the referral has been completed by SETMA’s referral department.
- Priority: either Routine, Immediate or STAT.
- Referral: Denotes the title of the referral and the provider to whom the referral is made.
- Referring Provider: The name of the SETMA provider who initiates the referral and to which the result of the referral will be returned.
Also the blue ‘T’ is a link to the tutorial for referral template. There are four places where the tutorial appears:
- Within the EMR
- Within SETMA’s Intranet
- Within SETMA’s Internet webpage
- Within manuscripts of all of SETMA’s tutorials
The Referral Template is opened by either:
- Double clicking in the Referral window
- Right clicking in the Referral window and clicking on "Add New."
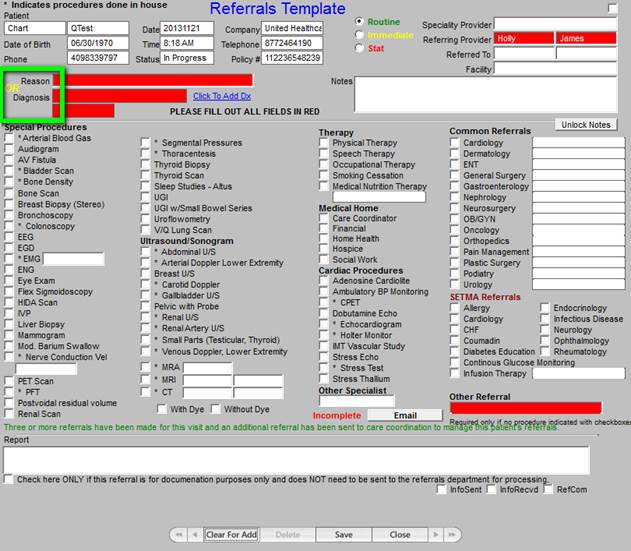
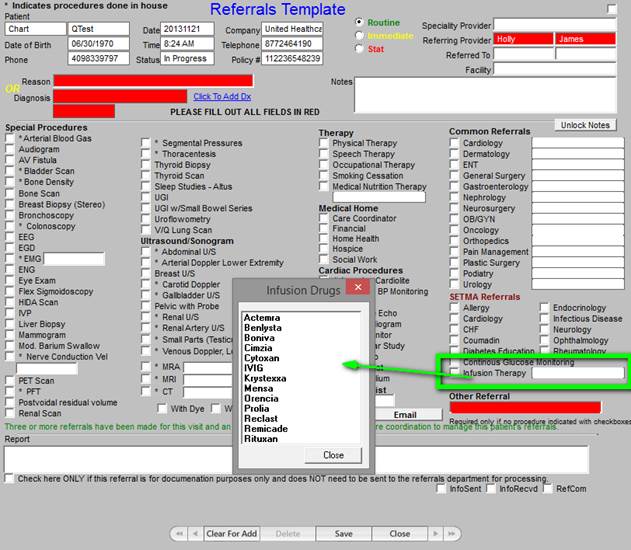
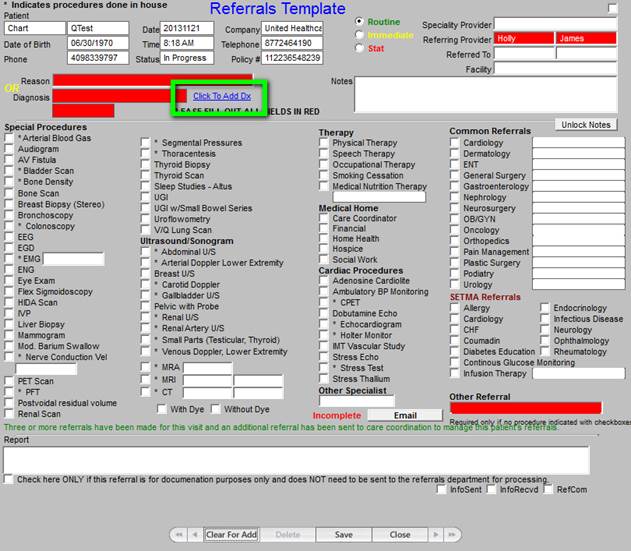
When the Referral Templates is accessed the following template will appear. The key to successfully using the Referral template is to make sure that you complete:
- The reason or diagnosis for the referral -- see below outlined in green. Note: all of the boxes in red are required fields and must be completed before the referral can be submitted to the referral department. Those fields are:
- Reason for referral or Diagnosis
- Referring Provider
- Other referral - if a referral is made which does not appear on the template - a description of the necessary referral must be place in this box before the referral can be submitted.
In order to select a diagnosis for the box of that name, you click on the button entitled “Click to Add Dx.” This launches the ICD-9 Code list and allows the correct diagnosis for supporting the referral to be added to the referral template.
- It is imperative that the provider specify a diagnosis. or condition, or question which motivated the referral.
- The reason field is a free text area which allows the placing of a specific questions into the referral template.
- If the referral is for a procedure or study, that must be indicated by checking the box by the appropriate study or procedure.
- Only one referral can be made with each template, this is to allow the auditing and tracking of each individual referral.
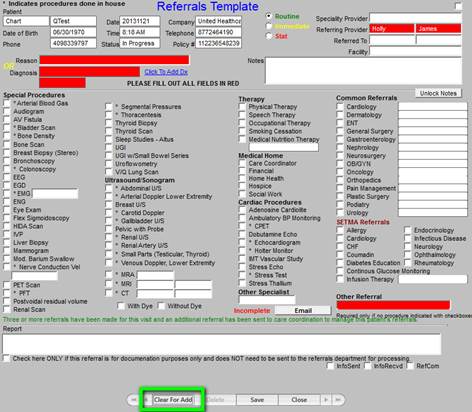
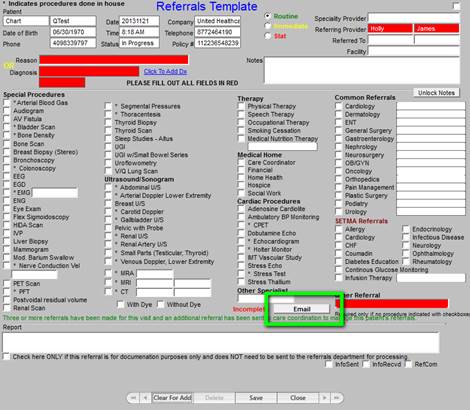
- If a second or third referral is being made in the same encounter, after you click the EMAIL button to send the first referral, you must click the "Clear for Add " button or close referral template and right click in the referral box and select Add NEW.
- Remember the EMAIL button has to be clicked after EACH referral.
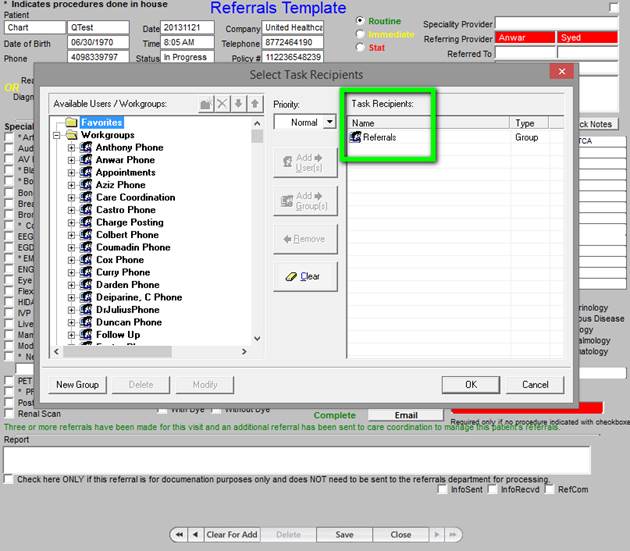
- Note: when the EMAIL button is clicked, the work group list pops up and referral group is already in the task recipients box just click ok and it is sent to the referral department.
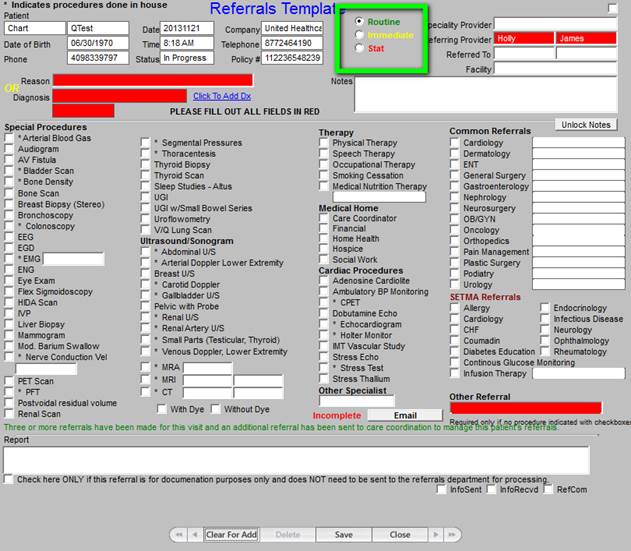
- After the EMAIL button is clicked you will see COMPLETE written in green to the left of the EMAIL button. (See Below)
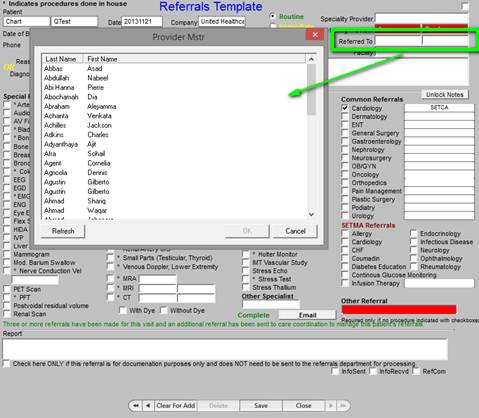
- To whom to the referral is being directed within SETMA, or for what the referral is being made. There are several options to from which to choose.
- Click in the ‘Referred To’ box and a list of providers will pop up. (see Below)
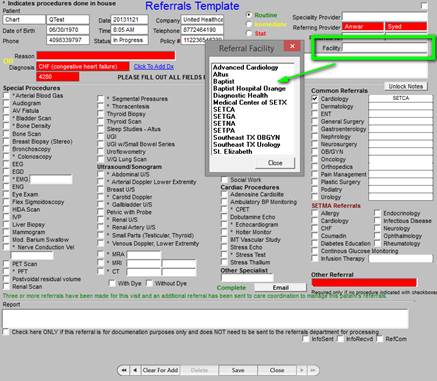
- Click in the Facility box and a list of facilities will pop up, click your choice. This box also allows free text, if the facility of choice of referral is not on the pop-up list.
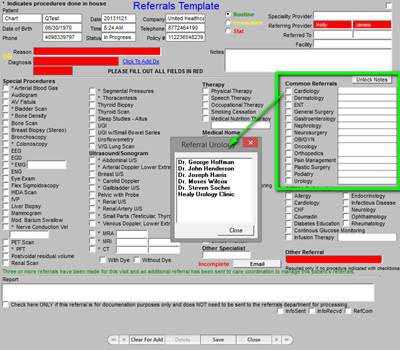
- The “ Common referrals section” lists the most common referrals and commonly used providers. Click the specialty that you want to refer to, click in the blank next to the specialty and it will generate a Pop Up list of the most common providers.
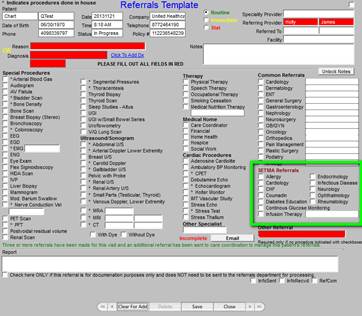
- SETMA Referrals section is for in-house provider referrals. If you click any of the choices in this section your referral will automatically go to the SETMA providers or clinic for that specialty. (note if you choose infusion you will see a pop up of medications available in the infusion clinic.) (See below)
- The urgency of the referral: routine, immediate, stat.
In order to complete a referral all areas in RED, must be filled in with appropriate information. Procedures with an * (asterisks) in front are test performed in-house.
Annual test such as mammograms, use notes area to indicate the facility where previous exam was performed.
Section on the bottom of the referral page is the area that the referral department documents on the progress of the referral process. 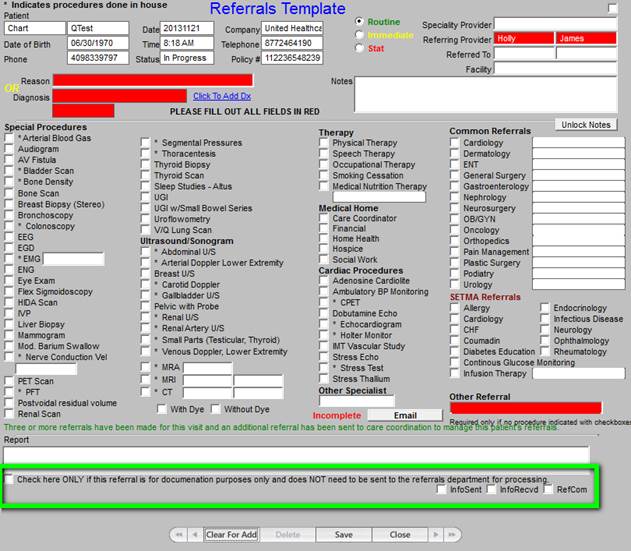
The box above outlined in green is used for the purpose of documentation on referrals made that do not require action by the referral department.
- InfoSent (Information sent) box is checked by referrals once information has been sent to the facility or MD for which a referral was requested.
- InfoRecvd (Information received) is marked by medical records once the reports are received and scanned in the patient’s chart. (This is completed by medical records.)
- RefCom (Referral complete) is checked by the referral department once all of the information (insurance, clinical and reason for referral) is sent to the facility, or MD for which the referral was requested.
|