|
April 23, 2010
Agency for Healthcare Research and Quality
Office of Communications and Knowledge Transfer
540 Gaither Road, Suite 2000
Rockville, MD 20850.
ATTN; Studies on Racial Disparities in Diabetes Care
Dear Sir:
Southeast Texas Medical Associates, LLP (SETMA, www.jameslhollymd.com) is a medium size multi-specially clinic in Beaumont, Texas. We have used a robust EMR (NextGen) since 1999 and have developed extensive disease management tools all of which are displayed on our website www.jameslhollymd.com under EPM (Electronic Patient Management Tools). We are also doing public reporting on multiple process and outcomes quality metrics published by NCQA (HEDIS), NQA, PCPI, PQRI, AQA and several developed by SETMA. The results of those audits are posted on our website un Public Reporting.
The reason for writing is in regard to your Atlanta Project concerning racial disparities in diabetes care. For our Patient Centered Medical Home, SETMA reports on comprehensive diabetes quality measures. There are four different measurement sets published by HEDIS, PCPI, NQA and PQRI. We report on all of them. In 2009, SETMA saw 3868 patients with diabetes and numerous others with pre-diabetes. We have active diabetes and hypertension prevention programs.
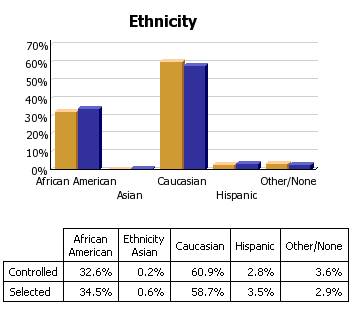
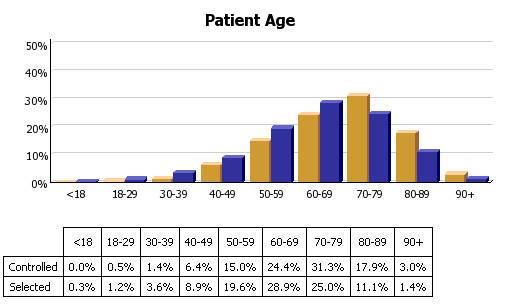
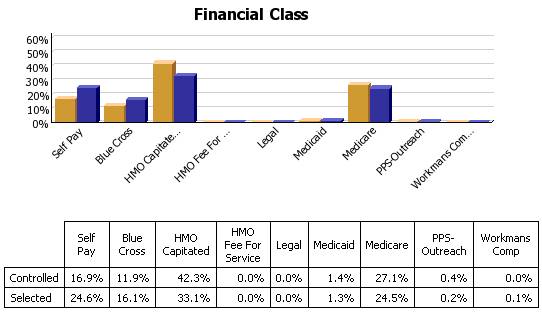
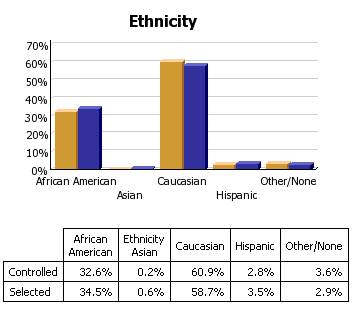
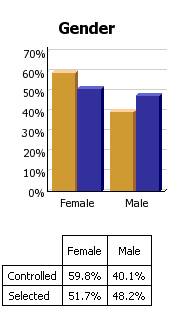
We have examined our data in regard to racial disparities as we had hoped to demonstrate that we have eliminated socio-economic and ethnic disparities in the treatment of chronic disease. Our data suggest that we have. The following is bar graph presentation of our data on diabetes. The gold bar represents the patients who are treated to goal (HgbA1C of 6.5% or lower) and the purple is those which are not. We have much more granular data on the distribution of our treatment which is presented below.
Our data shows that we have had progressive improvement in diabetes care every year between 2000 and 2009.
Year |
Median HgbA1C (%) |
Change (%) |
No. Tests Done |
2000 |
7.778 |
|
555 |
2001 |
7.4789 |
-0.299 |
1193 |
2002 |
7.4549 |
-0.024 |
3036 |
2003 |
7.2671 |
-0.188 |
4971 |
2004 |
7.2102 |
-0.057 |
7080 |
2005 |
6.9847 |
-0.226 |
7521 |
2006 |
6.8763 |
-0.108 |
8610 |
2007 |
6.6265 |
-0.250 |
9117 |
2008 |
6.5000 |
-0.1265 |
6275 |
|
|
|
|
Total Decline (2000 to 2008) |
-1.278 |
|
The history of SETMA's diabetes treatment is marked by three "breakpoints" - points at which there was significant improvement in the treatment outcomes for the population of patients we treat with diabetes. Historically, these were:
1. The designing and initiation of use of disease management tools for diabetes -- 2000
2. The inauguration of an ADA approved Diabetes Self Management Education (DSME) program in SETMA -- 2004
3. An endocrinologist joining SETMA. -- 2006
The statistical analysis of our data for 2009 compared to 2008 shows that we have continued to improve in our median values and that our goal of improving our standard deviation was achieved. The following is a statistical analysis of SETMA's HgbA1C data for the period March 2009 through March 2010.
|
Average |
Std Dev |
Median |
Mode |
Count |
Ahmed |
7.40 |
1.60 |
7.0 |
6.7 |
2121 |
Anthony |
6.87 |
1.55 |
6.4 |
5.9 |
407 |
Anwar |
6.70 |
1.24 |
6.4 |
6.1 |
652 |
Aziz |
6.95 |
1.68 |
6.5 |
6.4 |
285 |
Cricchio |
6.38 |
1.19 |
6.1 |
5.9 |
369 |
Curry |
7.12 |
1.77 |
6.6 |
6.1 |
185 |
Deiparine |
6.88 |
0.99 |
6.7 |
-- |
6 |
Duncan |
6.63 |
1.45 |
6.2 |
5.8 |
277 |
Groff |
7.22 |
1.45 |
6.9 |
6.2 |
31 |
Halbert |
6.79 |
1.75 |
6.3 |
5.9 |
616 |
Henderson |
6.72 |
1.50 |
6.2 |
5.9 |
269 |
Holly |
6.47 |
1.38 |
6.1 |
5.9 |
542 |
Horn |
6.67 |
1.36 |
6.3 |
5.8 |
300 |
Leifeste |
6.56 |
1.47 |
6.2 |
5.9 |
638 |
Murphy |
6.51 |
1.21 |
6.2 |
6.0 |
900 |
Satterwhite |
6.94 |
1.61 |
6.4 |
6.1 |
169 |
Sims |
6.36 |
1.32 |
6.1 |
6.1 |
238 |
Thomas |
6.48 |
1.47 |
6.1 |
5.8 |
343 |
Vardiman |
6.74 |
1.70 |
6.4 |
6.5 |
155 |
Wheeler |
6.54 |
1.23 |
6.2 |
5.9 |
288 |
Young |
6.68 |
1.65 |
6.2 |
5.7 |
144 |
|
|
|
|
|
|
SETMA |
6.82 |
1.52 |
6.4 |
5.9 |
8935 |
The following data is SETMA's HgbA1C for 2008.
|
PATIENTS with Diabetes ONLY |
|
ALL PATIENTS |
|
Provider |
Instances |
Average |
Std Dev |
Median |
Mode |
Latest Value Average** |
|
Average |
|
Ahmed |
2611 |
7.36 |
1.9081 |
6.8 |
6.0 |
7.25 |
|
7.36 |
|
Anthony |
1912 |
6.87 |
1.4698 |
6.5 |
5.8 |
6.72 |
|
6.88 |
|
Anwar |
3086 |
7.31 |
1.8300 |
6.8 |
6.2 |
6.92 |
|
7.29 |
|
Aziz |
1772 |
7.41 |
1.7623 |
6.9 |
6.9 |
7.29 |
|
7.36 |
|
Cricchio |
18 |
6.97 |
2.0353 |
6.1 |
5.6 |
7.05 |
|
6.79 |
|
Curry |
42 |
7.05 |
2.3711 |
6.0 |
6.0 |
6.76 |
|
6.92 |
|
Duncan |
1860 |
7.08 |
1.5776 |
6.6 |
6.4 |
6.71 |
|
7.02 |
|
Fowler |
1281 |
6.34 |
0.0495 |
6.3 |
6.3 |
6.03 |
|
6.12 |
|
Halbert |
2491 |
6.98 |
1.6540 |
6.5 |
6.0 |
6.80 |
|
6.85 |
|
Henderson |
1099 |
6.91 |
1.6533 |
6.4 |
6.2 |
6.80 |
|
6.85 |
|
Holly |
1701 |
6.99 |
1.6471 |
6.5 |
6.2 |
6.71 |
|
6.89 |
|
Leifeste |
533 |
6.44 |
1.2941 |
6.1 |
5.7 |
6.41 |
|
6.33 |
|
McClure |
1042 |
6.36 |
1.0143 |
6.1 |
5.6 |
6.21 |
|
6.36 |
|
Murphy |
1388 |
6.67 |
1.5915 |
6.2 |
5.8 |
6.67 |
|
6.60 |
|
Satterwhite |
41 |
7.14 |
2.3175 |
6.2 |
5.6 |
6.67 |
|
7.12 |
|
Sims |
60 |
6.87 |
1.8085 |
6.3 |
5.5 |
6.66 |
|
6.84 |
|
Vardiman |
1195 |
6.94 |
1.4570 |
6.6 |
6.2 |
6.58 |
|
6.76 |
|
Wheeler |
1173 |
6.90 |
1.7408 |
6.5 |
6.2 |
6.68 |
|
6.79 |
|
Wilson |
2092 |
6.97 |
1.4146 |
6.6 |
6.3 |
6.92 |
|
6.91 |
|
Young |
124 |
6.55 |
1.2147 |
6.2 |
6.0 |
6.51 |
|
6.20 |
|
Overall |
25521 |
6.99 |
1.6496 |
6.5 |
6.0 |
6.78 |
|
|
|
|
|
|
|
|
|
** Average value of each diabetic patients' most recent result. |
In early 2009, SETMA began a process which was directed toward continue our consistent improvement in the care of diabetes through 2009 and onward. The following is part of that discussion.
"As we move toward improving out mean and standard deviation of treatment of diabetes, we are looking for a new breakpoint for 2009. this breakpoint will be found by a combination of the first three, i.e.:
- A renewal of use by nurses and providers of the diabetes disease management tools which provide both guidelines for excellence and self evaluation tools for providers built upon the Consortium for Physician Performance Improvement data sets.
- A increase of utilization of our education department for ALL patients with diabetes treated by SETMA.
- An increased referral of not-at-target patients to Dr. Ahmed for specialty care.
"If our providers start utilizing the Diabetes Disease management program every time a patient with diabetes is seen, even if they are being seen for some other purpose, we will see our mean and standard deviations as an organization and/or as an individual provider decrease significantly over the next year. To that end, we are scheduling training sessions for all of SETMA's nursing staff to refresh our nurses knowledge of and utilization of the diabetes disease management tool. We will be auditing our nurses utilization of the LESS Initiate with all patients with diabetes, as well as their completion of the 10gm monofilament foot examination and the nursing portion of the Disease management tool.
"We will be empowering our nurses to initiate quality measures for patients with diabetes including:
- Referring patients to DSME if the patient has not had education in the past two years.
- Referring patients to endocrinology if their HgbA1C is, one, above 8 or two has not been improving over the past 12 months
- Referring patients to ophthalmology if they have not had a dilated eye exam in the past 12 months
- Ordering labs:
1) HgbA1C if it has not been done in the past three months
2) Lipids if they have not been done in the past twelve months
3) UA if it has not been done in the past twelve months
4) Thyroid profile if it has not been done in the past 24 months
5) Microalbumin if it has not been done in the past 12 months
- Complete the immunization with flu and pneumonia vaccine of our patients with diabetes.
- Encouraging our patients with diabetes to have a dental examination each year and referring them to a dentist if they do not have one.
- Recommending a baby aspiring a day
- Initiating the Lipid Disease management tool if they are not to goal with cholesterol
- Initiating the hypertension management tool if the patient is not to goal with blood pressure.
"We will also be establishing a monetary reward system for our nursing staff who achieve certain quality standards in these measures.
"To create this breakpoint prospectively rather than retrospectively seeing it through our data, we will be auditing our providers daily - and publishing those audit - as to the consortiums standards of excellence of Diabetes management. We will have training sessions with our providers to make certain that everyone knows how to use the disease management tools for diabetes, lipids, hypertension, cardiometabolic risk syndrome and the LESS Initiative (Lose Weight, Exercise, Stop Smoking).
I expect that in 2010, we will look back to a very successful 2009 in the treatment of diabetes and will see a fourth breakpoint in our data."
My purpose in writing is to make you aware of our work and to propose discussions between AHRQ and SETMA as to how to replicate our work elsewhere.
Sincere yours,
James L. Holly, MD
CEO, SETMA, LLP
www.jameslhollymd.com
The following are addition bar graphs and trending graphs of our diabetes reporting
Sincerely yours,
James L. Holly, MD
CEO, SETMA, LLP
www.jameslhollymd.com
| 