|
Abstract:
This presentation describes a method for maintaining excellent medical records through Chronic Problem List reconciliation. The process of Chronic Problem List Reconciliation involves the following six steps:
- The ability to select precise and accurate diagnoses from a robust electronic list.
- The ability to re-order the Chronic Problem List with the most important diagnoses at the top.
- The ability to highlight diagnoses in the Chronic Problem List which have not been assessed in a pre-determined period of time.
- The ability to archive resolved or invalid diagnoses in a retrievable fashion electronically with the date on which the diagnosis was archived.
- The ability to copy Chronic Problem List diagnoses into the Acute Assessment.
- Clear principles of Chronic Problem List Reconciliation.
Following these steps will enable complex care to be completed in an electronic medical record system maintaining an effective record for continuity and excellence of care.
Introduction
Medical Records are not an end in themselves, neither are they an exercise for the aggravation of healthcare providers. Medical Records are a method of communication between healthcare providers and patients for continuity, quality and consistency of care. In the outset, medical records were at best a silhouette of the patient’s care. They showed the broad outlines of the patient but with very little granularity. In the 19th Century, health records, when they existed, were brief acknowledgements of treatment or prescriptions, often kept on 3” by 5” index cards. In the 20th Century medical records increased in granularity reaching their pinnacle with dictation and transcription of healthcare delivery records which had a great deal of content. Yet, those records had the same flaws as 19th Century records. They were geographically bound, i.e., they could only be in one place at a time and one part of the record could not interact with another. Each episode of care was a separate record and the only continuity was when previous health information was included in the record of the current episode.
As the 21st Century approached with the explosion of medical information, all previous health record methods proved inadequate. After 1970, and more so in the first decade of the 21st Century health records became increasingly electronic. Electronic Medical Record (EMR) had the benefit of being accessible at many locations simultaneously. They were cumulative and documented patient care longitudinally. Increasingly, portraits of patient’s health care began to emerge, replacing the outlines of care or silhouettes.
EMR offered solutions to some of the most difficult problems associated with medical records. However, EMR created as many problems as they solved. On page 23 below, there are links to thirty five articles about EMR which SETMA has produced over the past fourteen years. Issues of security, confidentiality, content, interoperability, access, analytics and many more are addressed in these articles.
Perhaps the two most difficult issues in medical record keeping are the maintaining of:
- Valid and complete medication records and
- Valid and complete chronic problem lists.
Unfortunately, these two functions just happen to be the two most important parts of the record. Both issues are foundational to the fulfillment of the Triple Aim and to the achievement of patient safety. Because the chronic problem list is also critical for reimbursement, the sustainability of excellence in care, which is fundamentally an economic issue, the list is critical to quality outcomes. This is particularly related to HCC and RxHCC values (see HCC RxHCC Risk Tutorial for a full explanation of this system) which are important not only in Medicare Advantage, but also in Accountable Care Organizations work with Fee-for-Service Medicare and in Patient-Centered Medical Home.
The critical issues with problem lists are:
- The list must be produced from a robust ICD-9 and soon ICD-10 deployment from which diagnoses can be entered into the problem list, the assessment, disease management tools, referral templates and other parts of the EMR.
- The typing in of diagnoses, which will not work with billing and coding, or with sharing of data and analytics, is lethal to maintaining an accurate problem list.
- Upgrades to ICD-9 and certainly to ICD-10 include social codes such as “lives alone”, “Military Recently Deployed,” etc. There are also codes for such things as “Elevated CRP, etc, which allows you to maintain surveillance on conditions which are not presently under treatment but which need not to be forgotten and which need follow-up. While these upgrades allow for more granular documentation of the patient’s condition, they may produce a problem of growing Chronic Problem List which becomes unwieldy.
- Problem List Reconciliation require real time, routine review of the problem list with the ability to archive in a retrievable fashion diagnoses which are not currently active but which may become active in the future.
- Without these capacities the maintenance of the Chronic Problem List will be increasingly problematical.
Problem List reconciliation is a team effort including the following:
- Chart Maintenance - this is part of ever visit and every review of the patient’s chart.
- When the patient is seen the provider needs to review the problem list, as she/he must review the medication list. It is as if you have a “reconciled” medication list and a “reconciled” problem list at each visit.
- When data, information, tests, procedures, etc., are received on a patient from another provider or organization the clerk has to be given the authority to add diagnoses to the chronic problem list. Then when the patient is seen the provider reviews the diagnoses and determines whether it should remain in the list or not.
- It is ideal if it is possible to reorganize the chronic problem list in order of priority. SETMA has designed a system where it is easy to do this in a matter of seconds even with 18 diagnoses. Thus, the most important diagnoses can appear at the top of the list such as Diabetes, Renal Disease, Prostate Cancer and less critical but important diagnoses can appear last such as “Elevated Sed Rate”, “Hx of Tobaccoism”, “Family History of Diabetes”, etc./ .
2. Chart Reviews - nurses charged with going through charts:
- Making certain that for important diagnoses that there is history, physical, testing, etc., information to support the diagnoses and calling it to the provider’s attention if it is not there .
- Reviewing consultations, procedures, etc., to make sure that all valid and accurate diagnoses have been entered into the chronic problem list so that they can be brought to the attention of the provider.
- Making sure that all diagnoses are entered electronically and not by typing so that they interact with the disease functions of the system.
3. Quality Improvement - healthcare providers reviewing the charts of other providers
- The same kind of review is done by the provider during a patient encounter and the nurse with chart reviews, but it is more focused on the quality of care based on the documentation in the record and the completeness of the chronic problem list. This is most often done with new providers, or with providers having problems with their documentation.
- After these reviews a face-to-face or a written conversation is had with the provider to address deficiencies.
General Principle: Reconciliation of medications or of chronic problem lists is hard work and must be a priority, if it is going to be done well and consistently.
Tutorial for SETMA’s Chronic Problem List Reconciliation
- Electronic Access to a robust list of diagnoses which is intuitively organized.
(Disclaimer: For fourteen years, SETMA used a “home grown” ICD-9 Code list. With the advent of ICD-10 and SNOMED, it was necessary to update our system to a proprietary list. SETMA has no financial interest in the company whose product we selected and we are not paid by this company. We have nothing to disclose. There are other vendors which can be used.)
The tool which SETMA employs is integrated with our EMR. This tool has taken the 15,000 ICD-9 codes and expanded them to a list of 100,000 codes by naming each code in multiple fashions to make it easy to access the correct code. This transition will enable SETMA, we think, to utilize the 150,000 ICD-10 codes more efficiently and more effectively.
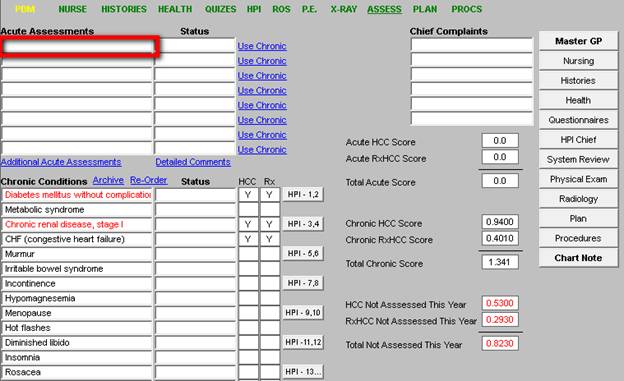
The following is how we use the tool, by clicking in the Assessment space, the tool is launched. In the space below, outlined in red, you would type a name or abbreviation, such as “CHF.”
This then launches a list of codes which fit that description.
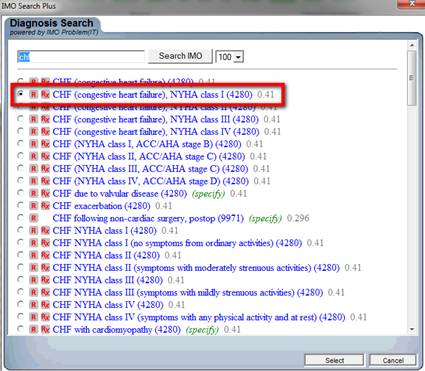
Once the correct code is identified, the radial button next to it is marked and the button entitled “select” is clicked (see below).

This places the code description on the assessment screen.
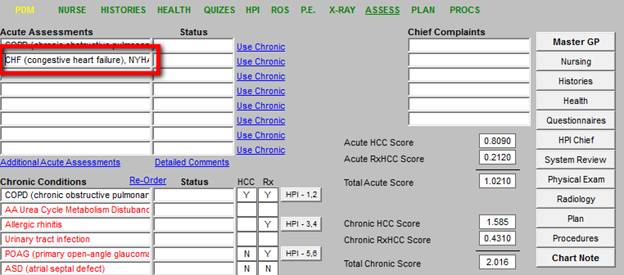
The tool we selected also notes whether the diagnoses is a HCC and/or an RxHCC and the coefficient assigned to that diagnosis is listed. Each is outlined in red below.
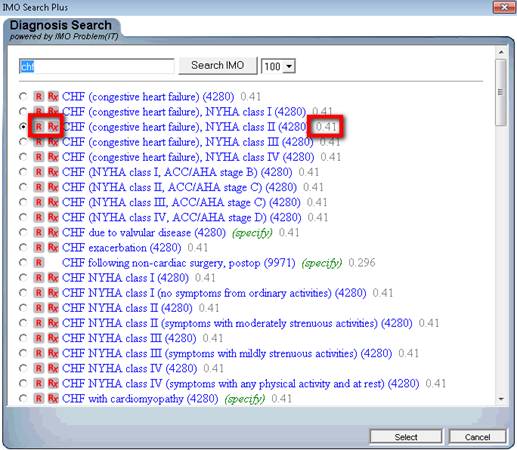
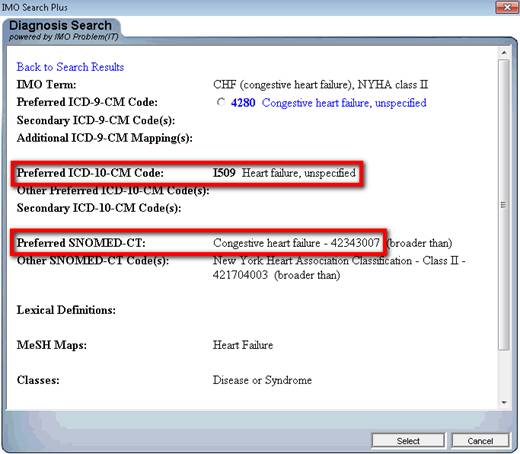
Our tool for ICD-9 Code selection already has ICD-10 and SNOMED cross linked as is seen below. In 2014, when ICD-10 is launched, our use of it will be simply a change at the server level of our EMR. The same will be true for SNOMED.
In this same way diagnoses can be added at many different places in addition to the Acute Assessment, including:
- Chronic Conditions
- Plan
- Referrals
- Disease Management tools
Valid and complete Chronic Problem Lists are critical to excellence of care because if a diagnosis is out of mind, it will not be evaluated. One of the audits SETMA does is to look at all diagnoses which are identified in the hospital medical record. To do this, all of the following are reviewed:
- Daily progress notes
- Procedures
- Laboratory values
- History and Physical examinations
- Consultant notes
- Surgical notes
- Etc.
The Discharge Summary (renamed by SETMA as “The Hospital Care Summary and Post Hospital Plan of Care and Treatment Plan”) is reviewed to see how many of those diagnoses are not in this transition of care document. Any diagnoses not in the hospital summary will routinely be overlooked in follow-up.
The great value of documenting hospital history and physical examinations and Hospital Care Summaries and Post Hospital Plan of Care and Treatment Plan in the same EMR data base is that the documentation element of care continuity is seamless. When the hospital record is completed with all admitting morbidities and co-morbidities, the follow-up of the patient is made straightforward and complete.
| 