|
Our February 17, 2009, column introduced the concept of Medical Home, but "What is it?" Two things are novel and may be the energy behind Medical Home. First, the patient and the healthcare provider enter into a collaborative relationship where the more the patient knows and understands about his/her health, and the more the patient accepts and takes responsibility for his/her health, the closer they come to forming a healthcare team which is defined by the concept of Medical Home. Second, Medical Home not only results from this team formation but also from the healthcare provider, who is identified by the patient as his/her principal healthcare provider, having information about the patient which is:
- Comprehensive - this information goes beyond the routine medical, social, family and habits history and includes things such as the living condition, literacy, nutrition, etc., of the patient.
- Accessible - this information must be readily accessible to the provider.
- Considered in medical decision making for the patient - this information must be an active part of the patient's care and evaluation.
Historically, medical records and medical databases have looked more like a stick-figure than like a portrait of the patient. Electronic patient records have enabled that portrait to take on granularity and specificity so that the "picture" of the person is more personal. Now, Medical Home requires that that portrait take on the unique features of the patient which are personal, specific and unique. Creating the database for this information-set is the "first thing." Making that database interactive and dynamic is the "second thing." Using that database in an active and inter-active means in the care of patients is the "third thing."
Under the Medical Home model the provider has NOT done their job when they simply prescribe the care which meets national standards. Doing the job of Medical Home requires the prescribing of the best care which is available to the patient. For example, a year ago, the partners of SETMA formalized a 501-C3 not-for-profit foundation - The SETMA Foundation - which has as its purpose medical education and underwriting the care for patients who cannot afford care. Obviously, this fledgling foundation has limited assets but it is a beginning.
Recently, I saw a patient who has a very complex and fascinating healthcare situation. During his office-based hospital follow-up, I discovered the patient was only taking four of nine medications because of expense. I believe in this case, SETMA practiced Medical Home as the patient left the office:
- Appointment to SETMA's American Diabetes Association-approve diabetes-education program. The fees for the education program were waived. However, while talking to the patient's family, I discovered that the patient could not afford the gas to come to education meetings. The patient also left with a gas card with which to pay for the fuel to get the education which is critical to the patient's care.
- My staff negotiated a reduced cost with the patient's pharmacy and made it possible for the pharmacy to bill The SETMA Foundation.
- Because the patient cannot work at his job, the patient's care also involved counseling that we will coordinate an application for Social Security disability.
Are gas cards, disability applications, paying for medications a part of a physician's responsibilities? Absolutely not, but are they a part of Medical Home? Absolutely. This patient, who was depressed and glum in the hospital, such that no one wanted to go into the patient's room, left the office with a smile and feeling that there is hope. It may be that the biggest result of Medical Home is hope.
Now, every healthcare provider doesn't have a foundation and even ours can't meet everyone's needs, but assisting patients in finding the resources to help our patients will be a part of medical home. And, when those resources cannot be found, Medical Home will be "done" by modifying the treatment plan so that what is prescribed can be obtained, for the ordering of tests, treatments, prescriptions which we know our patients cannot obtain is not healthcare even if the plan of care is up to national standards..
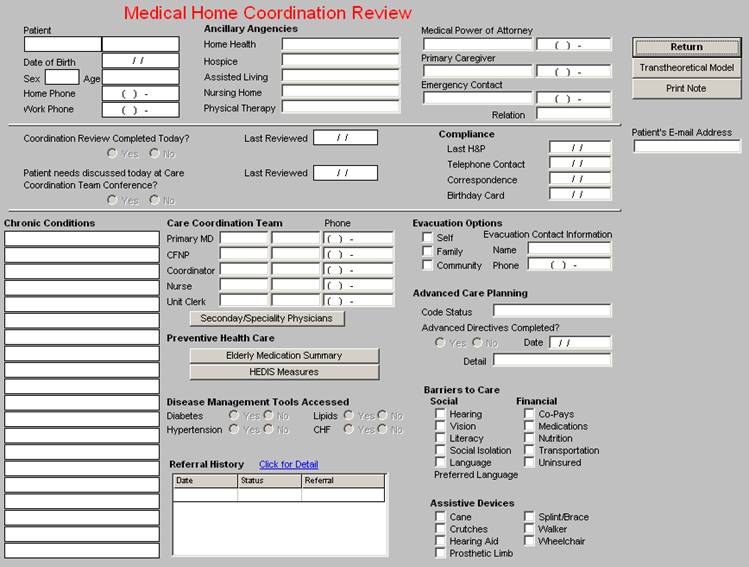
Medical Home Coordination Review
This is a quick look at what a Medical Home Coordination Review would look like. Almost all of the data will be collected from other data fields which already exist in our EMR. The final product will be interactive. Notice the team concept, along with the coordination of care initiatives, particularly for things such as evacuations and emergencies. This template will assume three kinds of coordination of care contacts: telephone, mail, and office visits, with a possible fourth, e-mail. The disease management tools are the ones being used in this patient (not a real patient). While the screen shot does not show the functionality, if you click on the Preventive Health and HEDIS buttons, a pop-up appears and tells you what measures are up-to-date and which ones are not.
As we have thought more about Medical Home, it occurs to us that the dynamic and the potential of Medical Home is found in its name. What is a "home:"
- It is a place where you need fear no harm from those who are with you.
- It is a place where your needs are met.
- It is a place you can go when you don't know what else to do.
- It is a place where you can be yourself and you can tell others how you really feel without fear of rejection.
- It is a place where others really want to see you succeed.
- It is a place where if you are away too long, someone is calling to find out if you are OK.
- It is a place where you are treating like family.
Coupled with excellence of care, Medical Home has the potential for leveraging great benefit for patients and providers from the healthcare delivery equation. Like the homes in which we grew up, Medical Home will facilitate the success of the patient in a nurturing environment.
Goodbye Mr. Chips and Medical Home -- The value of a life given to the service of others
Recently, I saw the last few minutes of Goodbye Mr. Chips. Based on a novel by James Hilton and originally published in 1934 - Hilton was also the author of Lost Horizon which was about the mythical Shangri-La - the movie was released in 1939. Another version was released in 1969 starring Peter O'Toole. The novel, Goodbye Mr. Chips, is very similar to my favorite British novel entitled, To Serve Them All of My Days, by R. F. Delderfield, published in 1972.
I never see this movie without being deeply moved by the value of a life given to the service of others. The story is about Mr. Charles Chipping played by Robert Donat. Chipping comes to be called "Chips" by the boys in the boarding school where he teaches and where, during WWI, he becomes the headmaster. As he dies, Mr. Chips is dreaming of all his past students. He over hears two colleagues lament that he is dying alone and that he lived a lonely life without his own children. He awakens and says that he has not lived alone. He has had thousands of children, "All boys, he declares." In the last scene, young Peter Colley III, the youngest of a family of boys whom Chips had taught through the years, waves to him and says "Goodbye, Mr. Chips, goodbye."
Dr. Robert Culpepper and Medical Home
It occurred to me, as I was again moved by this dramatic scene, that Chips' attitude toward the boys is the same spirit and attitude which will be at the core of a Medical Home. And, in that regard, the new idea of a Medical Home really is only re-discovering the "old way" of medicine from 50 years ago. When I graduated form medical school in 1973, I called Dr. Robert Culpepper in Pineville, Louisiana. He had been my family's doctor from 1940 until we moved to Natchitoches, Louisiana in 1949. He lived in a fine home atop a beautiful hill which was on the way to my grandparent's home. Each time I passed that home through the years, I thought of Dr. Culpepper.
When I graduated from medical school, I wanted to let him know. When I called him, retired and now quite elderly, Dr. Culpepper, who had not seen my parents for over 24 years, said, "Larry, how are Bill and Irene," calling my parents by name. While in my mind, my parents were large, they were not wealthy or prominent people, yet he remembered their names and expressed personal interest in them, just like a "family" would. That is a response which reflects the dynamic of a Medical Home.
Medical Home is an old idea reinvented with technology attached - Generative Thinking
As we design electronic support for the implementation of this "new" idea (Medical Home), we shall remember that it is really quite old. It is like many things in which the activity of creating the future is simply an effort to make that future resemble the best of the past. And, in that creating process, we must employ what Dr. Peter Senge calls "generative thinking" in his seminal work entitled, The Fifth Discipline.
Medical Home requires that patients become people and that those people have personal value to us beyond their financial contribution to our success. While this is most often the case with all physicians and healthcare providers, there are special obligations which its formalization in Medical Home imposes upon the provider, which if they are not systematized are often overlooked. This is why it is possible to have implemented all of the elements of Medical Home excellently without having become a Medical Home. Medical Home must have a foundation of excellence in the science of medicine but that excellence must be received in a personal setting.
As we understand what Senge calls "generative thinking," we with the collaboration of others will create this future we call Medical Home and in doing so we will create a future which produces our best result and which fulfills our best goals and ambitions as healthcare providers. Of generative thinking, Senge said:
"This then is the basic meaning of a learning organization...continually expanding its capacity to create its future. For such an organization, it is not enough merely to survive. 'Survival learning' or what is more often termed 'adaptive learning' is important - indeed it is necessary. But for a learning organization, 'adaptive learning' must be joined by 'generative learning,' learning that enhances our capacity to create.
"As I began my doctoral work...I felt that the solutions to the Big issues lay in the public sector. But I began to meet business leaders...These were thoughtful people, deeply aware of the inadequacies of prevailing ways of managing. They were engaged in building new types of organizations - decentralized, nonhierarchical organizations dedicated to the well being and growth of employees as well as success. Some had crafted radical corporate philosophies based on core values of freedom and responsibility...Gradually I came to realize why business is the locus of innovation in an open society. Despite whatever hold past thinking may have on the business mind, business has a freedom to experiment missing in the public sector."
"Medical Home!" A daunting concept. As SETMA moves into this new era of medicine, we will look forward to the health benefit to our patients, who really are like our professional family and we believe this will have great benefit to our community.
| 