|
It is important to keep the title of this article in mind as you think about the new outbreak of Ebola in the Congo. It is highly improbable that the outbreak will spread internationally, but we will be prepared if it does. Ethically, however, we should be as concerned for the welfare of those imminently facing this danger as we would be if we faced it here.
In 2014, the world’s health attention was focused on Africa. Over 11,000 people died from Ebola in that outbreak. Investigators determined that two considerations delayed the World Health Organizations response to this crisis: one, they did not want to spread panic; two, they did not want to offend African nations. This time the WHO has not been so timid in their response. On May 17th, it was confirmed that fourteen cases of Ebola had been confirmed in the Congo. There have been 40 suspected or probable cases including 25 deaths are being investigated.
Over 500 people, who are thought to have been in contact with the known cares are being sought. This week it has been confirmed that Ebola has spread to Mhbandaka, a city of over 1 million people. As of last Friday, the WHO has declined to this an international emergency.
In March 2014, WHO announced the discovery of Ebola in West Africa's Guinea by posting a two-sentence update on its website. Over the next few months, the number of victims spiked, cases spilled across borders and international aid workers became infected. Despite calls to declare the raging epidemic a global emergency, WHO resisted: Not until 1,000 people had died did it convene its expert committee to even consider the possibility. Ultimately, more than 11,000 people died in West Africa.
There are differences in this outbreak. The West Africa Ebola outbreak isn't entirely comparable to the current situation in the Congo. When the lethal hemorrhagic fever broke out in Guinea, it was in a region with porous borders that had no experience with the disease. In comparison, Congo has had more Ebola outbreaks than any other country in the world, and although the virus made it to a big city this week, most of the cases appear to be in a remote area accessible largely by dirt roads.
From a humanitarian perspective the comfort level with this outbreak is not well considered as it is still affecting human beings who need the world’s help.
Because of our 2014 experience in the United States and in Texas, we are well prepared to recognize potential threats and to respond to them effectively. The same limitations to SETMA’s involved would apply today as applied four years ago. In the case of another outbreak in the USA, SETMA will collaborate with the Jefferson, Orange, and Hardin County Health Departments and the Texas Department of Health and the Centers for Disease Control, but SETMA will NOT be the place where a person who fears they have been exposed to Ebola, or worse, fears that they may have Ebola, should seek care.
In 2014, SETMA enunciated the following principles which are still valid:
- If you think that you have been exposed to Ebola or that you have Ebola, you should isolate yourself from others and call the County or State Health Departments. .
- If you have been exposed to Ebola, or if you have traveled in West Africa in the past thirty days, you should isolate yourself in your home and call those agencies and get specific directions of where to go.
- With every person, we want to accomplish two goals: to give you the best care in the most appropriate setting possible and to prevent Ebola from spreading to others. The first is a personal responsibility to oneself; the second is an ethical responsibility we all have to each other.
SETMA’s Preparation for Ebola
In 2014, within two days, SETMA had deployed and deployed the following electronic medical record response to Ebola. Once the threat ended four years ago, these templates can be reactivated in a few minutes if the need arises.
Outlined in Green are the questions which help us be sure that no one is overlooked. In SETMA’s EMR these are “must answers.” That means that when a nurse or healthcare provider accesses a medical record, they cannot proceed until one or more of these responses have been documented.
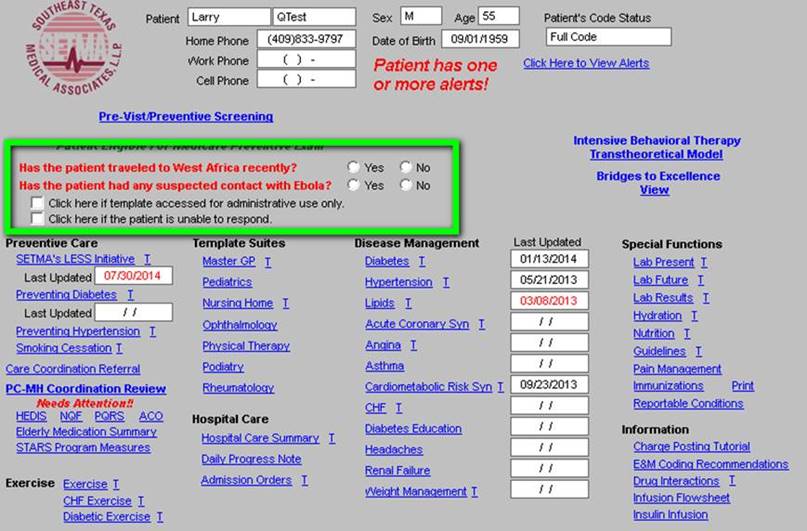
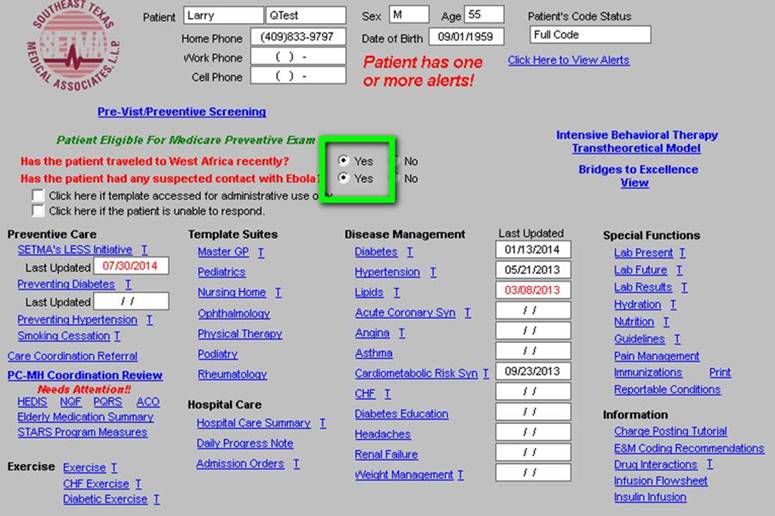
Both questions written in red and outlined in green must be answered before the provider or nurse can continue with the patient visit. SETMA is aware that it is unlikely that we will ever be confronted with a patient who has been to West Africa, or who has been exposed to someone with Ebola, but because of the petrochemical industry and the travel in Africa associated with their employs, the potential for that exposure is higher than in some areas of our country. If the answer to both questions is no, then the provider and nurse continues with the healthcare visit. If the answer to one or the other is “yes,” a list of instructions appears. (see below)
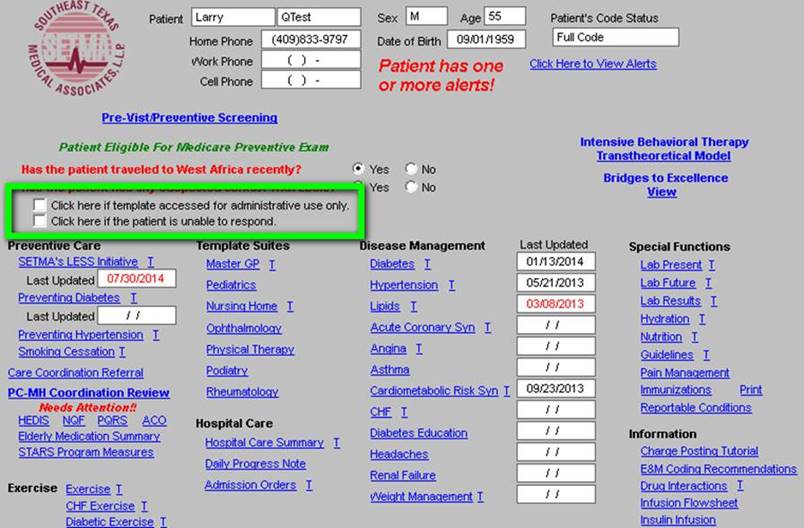
There are other occasions which are compliant with healthcare privacy laws and HIPPA when a patient’s chart must be accessed. Because, these questions must be answered before anyone can proceed past this point, two options, outlined in green below, have been added in order to allow appropriate responses to be made.
If the answer to either question in red on the first template above is “yes,” the following template in bright yellow will appear.
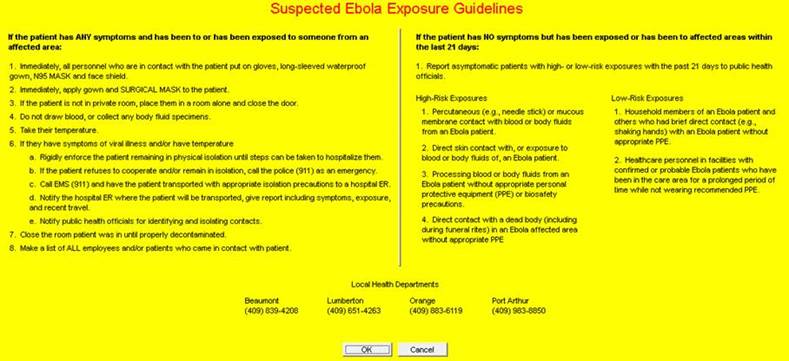
These guidelines do not involve the treatment of Ebola positive patients, or even the testing of patients who are suspected of having Ebola exposure or infection. These measures are for the identification of patients who may have been exposed to and/or infected with Ebola, getting them to a proper site for treatment and/or isolation, without exposing others or putting suspects at increased danger of not getting the proper care. Again, we see the two fold goal: proper treatment and care of the individual and proper protection of the pubic from the spread of the disease.
Further, if another outbreak should occur, and at present we do not anticipate such; SETMA would take the follow steps immediately:
Training: We would train all staff and employees. We train unit clerks, nurses, and registration staff to make certain that there are no exceptions to the screening and surveillance of Ebola risk.
Protection: SETMA would immediately have the necessary Personal Protective Equipment (PPE) at each clinic. This would not be the very elegant “hazmat” suits which have so dramatically been displayed on television. It will include masks, eye protection, gloves, gowns and shoe protection for staff and patients involved in the incident. (“Hazmat” -- a material flammable or poisonous or infectious that would be a danger to life or to the environment if released without precautions)
Protocols: Once anyone is identified as having potential exposure, every effort will be made to prevent the escalation of the category of risk. No blood or other biological specimen (sputum, urine, feces, vomitus, etc) will be collected. The suspect will be isolated in a room with appropriate instructions and support. Only one SETMA staff member will interact with the suspect until the proper steps have been taken to secure them.
Preparation is the best Protection
One of the principles of life is that “if you are prepared, the thing for which you prepared seldom occurs,” but if you are not prepared if invariable will. The time will come when the Ebola crisis will subside and probably disappear. Another principle is that you are not only responsible for you own health but you are ethically response not to become a hazard to the health other others.
Potential Benefits of the response to Ebola and Herd Immunity
Herd immunity occurs when 80-90% of a population has a theoretically protective level of antibodies, either from mounting an antibody response to an antigen in a vaccine or from suffering through a virus and recovering. Only 30-40% of people get the Seasonal Flu vaccine - far short of herd immunity. If everyone realized that as with Ebola, they have a personal healthcare responsibility to be protected and to take responsible actions but that they also have an ethical responsibility to their community and their nation, it may be possible to gradually increase the percentage of people who are immunized until we reach “herd immunity” standards.
It is SETMA’s hope that the fear of Ebola and the demand for vaccines for this dreaded disease will allow us to “spread the word” that Influenza A and B and Pertussis (Whooping Cough) and other infectious diseases kill hundreds of thousands of people throughout the world every year and that we have excellent vaccines for these infectious diseases. These vaccines are greatly underutilized with less than 35% of people in the United States taking a “flu shot” every year. If 90% of Americans took their flu shot every year, the flu epidemic would be very mild, the number of deaths would decrease dramatically and the general health of the population would improve.
| 