|
Cardiovascular risk assessment is important in your healthcare planning. For more detail review the fourteen-part series published in 2005; the following is the link to that information: Cardiovascular Disease Risk Factors
Even though these articles were prepared eight years ago, they are still valid as a foundation for you understanding your risk of developing heart disease.
At a minimum, once you are over 45, your annual cardiovascular risk assessment should include:
- Cholesterol and Triglycerides, particularly your low density lipoprotein (LDL, the bad cholesterol) and your high density lipoprotein (HDL, the good cholesterol).
- A calculation of your Framingham Risk Scores - there are twelve.
- An assessment of your “what if scenarios.” This is a recalculation of the Framingham Risk Scores, if you improve the elements of a score to goal, or to 20% of goal.
- Cardiometabolic Syndrome Risk Assessment
- A calculation of your Fredrickson Classification of Dyslipidemia, if relevant
- An assessment of other conditions (called co-morbidities) which contribute to cardiovascular risk, such as diabetes, hypertension, obesity, inactivity, smoking, etc.
- Evaluation of your activity level, weight assessment and exposure to tobacco smoke.
- Screening for hypertension and diabetes.
Beyond the routine determination of your cholesterol, HDL, LDL and Triglycerides, it is possible to do more detailed evaluation of your cholesterol profile with other tests, one of which is the Vertical Auto Profile (VAP). Generally, this test is not paid for by insurance but is helpful in special circumstances. The following is an explanation of when this test would be helpful. As is obvious, the ‘special” circumstances in which this test is helpful are fairly common. They are:
- Any patient with established atherosclerosis vascular disease
- Any patient with diabetes mellitus
- Any patient with a Framingham risk score over 5%
- Any patient with an elevated inflammatory biomarker
- Any patient with NCEP ATP III risk factors:
- Cigarette smoking
- Hypertension
- Low HDL-C (<40 mg/dL)
- Family history of premature CHD
- Age (men >= 45 years; women >= 55 years)
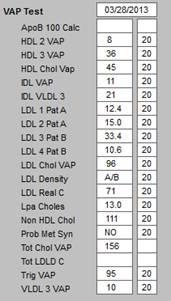
The following is a VAP result from a real patient whose major concern is a strong family history of premature coronary heart disease. It’s comparison with the routine cholesterol results shows how it can be helpful to “know more.” In this case the “routine cholesterol” testing would have only shown results of:
- Cholesterol 136
- HDL 45
- LDL 96
- Triglycerides 95
The Cholesterol/HDL ratio in this case is 3.0. In that we want that ratio to be below 4.0, the routine cholesterol test would give us confidence that this patient has low cardiovascular risk. An HDL of 45 in an adult male is very good. But the routine test does not give the full picture. We know that there are several different particles measured by HDL; there is HDL2 and HDL3. It is the HDL2, which is most protective against heart disease. With the VAP test, we know that the HDL2 is a small part of this patient’s total HDL. In and of itself, this is not alarming, but it is a caution.
Apolipoprotein B (ApoB) is a measure of the “bad” cholesterol. The lower the ApoB, the better. This patient’s ApoB is 82 which is normal. But the over all test shows a mixture of A/B (A = Apolipoprotein B - “bad”; B =Apolipoprotein A - “good”) for the LDL Density. Once again, this is not alarming but is a caution.
The real benefit of the VAP in this case is the reporting of the Lpa (spoken as “Lp little a”). The 13.0 value is higher than is desirable in that the Lpa is a very strong indicator of cardiovascular risk. With the low HDL2 and the moderately elevate Lpa, even with the Cholesterol/HDL ratio being good, it would not be unreasonable to recommend that this patient take a low dose statin to mitigate the low HDL2 and the elevated Lpa.
In that cardiovascular disease is an inflammatory process, it is possible to determine whether a patient has abnormal “inflammatory markers,” which shows them at high risk of cardiovascular disease on the basis of inflammation. Due to a high risk of cardiovascular disease in this patient’s family, not only was a VAP test done, but other tests were done for the presence of inflammatory markers. Next to the marker is the result in this patient’s evaluation:
- Ferritin - 356 which is high
- Fibrinogen - not done
- Homocystiene -- .13 which is mildly increased.
- hs-C-reactive protein -- .9 which is normal
- PA-1 (Plasminogen Activator - less than 5 which is normal.
- Uric Acid - not done
- White Blood Count Elevation - 7.9,000 which is normal
In order to assess you for risk of diabetes, we completed a Hemoglobin A1c on you. Your value is more than normal, is it excellent. This indicates that you do not have diabetes and you are a very low risk of developing diabetes.
Another measure of cardiovascular risk is the Calcium/Magnesium ratio. This patient’s calcium is slightly high; in his case due to his taking a large dose of calcium (Ca++) each day. Calcium works in the body to promote clotting. This patient’s magnesium (Mg++) is also slightly high. Magnesium works in the body to promote the breaking up of blood clots. There must be a balance between blood clotting and blood not clotting in the healthy person. One indicator of this balance between clotting and not clotting is the Ca++/Mg++ ratio. When the ratio is 4, or below, it is ideal. In this patient’s case it is 5.5. This would suggest that the patient’s blood would have a greater tendency to clot which is not good.
The following are the recommendations made to this patient.
- For the slightly elevated homocystiene, I mg of Folic Acid a day would be appropriate.
- For the elevated calcium, stop the calcium you are taking.
- Particularly with an elevated Ferritin (normal is below 325), we would like to control your calcium in order to improve your Ca++/Mg++ ratio.
- The hsCRP is normal and the Hemoglobin A1C (HbA1c) is normal both are good.
- The fasting insulin is 8 and your fasting glucose is 85. Both are excellent and with these two values we are able to calculate your HOMA-IR (Homeostasis Model Assessment of Insulin Resistance) which is 1.7. All of these values mean that you neither have diabetes or pre-diabetes, and that you are at a very low risk of developing diabetes..
- Your Plasminogen Activator Inhibitor I (PAI-1) is normal. This test is not often used in clinical practice, but is a very good inflammatory risk factor.
Your Framingham Risk Scores are excellent. Calculation of the Cardiometabolic Risk Syndrome shows that you do not have insulin resistance or careiometaboic risk. You do not have a Fredrickson Dyslipidemia. In the face of all of this, even with your family history, you have a very low cardiovascular disease risk.
With the elimination of the extra calcium, the addition of the folic acid, the monitoring of your Ferritin, the repeating of your calcium/magnesium ratio in two months and the continuation of a low-dose statin, your mild inflammatory risk should be totally mitigated. If we had not done the VAP test, we would not know this, but with these test results, we are able to give you a more nuanced recommendation for your future healthcare.
| 