|
AHRQ is the Agency for Healthcare Research and Quality. It is a department of the Centers for Medicare and Medicaid Services. Recently, SETMA has had a dialogue with AHRQ about ethnic disparities in health care. The following is a June 3, 2010 letter to AHRQ.
Thank you for your response to my letter. I have previously reviewed AHRQ's website and the information on disparities in care at http://www.ahrq.gov/research/dispmtgsum09.htm.
One of our major quality initiatives this year is to totally remove ethnic disparities in the care of diabetes, hypertension and dyslipidemia. Our experience is that several issues contribute to the disparities. These include:
- Access to care which is a healthcare structure problem. This includes the lack of insurance and/or inadequate insurance. Also, it includes the lack of healthcare providers who are willing to take on complex patients. And, as is illustrated below, it sometimes is the result of Health and Human Services rules through CMS which creates gaps in care.
- Co-morbidities particularly obesity, tobacco, inactivity and sometimes alcohol.
- Personal resources which limit access to gymnasiums, healthy nutrition, education, medications, etc.
- Cultural predilection for foods and habits which contribute to many of the above.
- Limited access to dental care.
- Fragile social, economic and health infrastructures.
Almost all of these were illustrated in my clinic this morning. A patient with whom I have been working to control diabetes with ophthalmological complications, hypertension and dyslipidemia, announced that he lost his Medicaid coverage. This was due to the fact that his Social Security disability has been approved. His new income made him ineligible for Medicaid but Medicare benefits are delayed for two years. Untreated and uncontrolled diabetes for two years could devastate his health. This gap in insurance coverage needs to be correct by HHS.
In two years, this gentleman will be eligible for Medicare benefits, but for the next two years he cannot afford healthcare including medication. He said he would have to go back to the local indigent clinic. As SETMA has morphed itself into a Patient-Centered Medical Home, we have accepted responsibility for not only prescribing the best treatment dictated by evidenced-based medicine, but also for working to help our patients access the care we prescribe. While we want to measure and improve the care of large populations, we never want to lose sight of the individual. Populations are made up of persons and they are each unique people.
As a result of our commitment, Southeast Texas Medical Associates, LLP (SETMA) created The SETMA Foundation. Though the Foundation, we have resources with which to support this patient's care until he receives his Medicare benefits. Last year alone, SETMA's partners contributed $500,000 to the Foundation in 2010, the partners contributed another $500,000 to the Foundation in 2011. Between this patient not being charged for office visits or laboratory work, and the Foundation helping with his obtaining all of his medication, we can continue to work with him to preserve his vision, his kidneys and to protect his heart and arteries. The fact that he is African-American is of no consequence except that it illustrates another way in which we are help resolve ethnic disparities in care.
The SETMA Model of Care
Through SETMA's COGNOS Project (see www.jameslhollymd.com, Your Life Your Health, "COGNOS Project" for details), we are able to analyze our care for diabetes, hypertension and dyslipidia, as well as other conditions such as CHF, Renal Disease, etc. (for more on this see the article referenced below entitled The SETMA Model of Care - Diabetes Precision Medicine, Quality Performance)
In addition to ethnicity, through COGNOS, we analyze the following. (We can analyze by the entire clinic, by each location, by each provider or by contrast any subgroup for all of the following):
- Mean, Mode and Median along with Standard Deviation of treatment goals for each, i.e., HgbA1c, LDL, Blood Pressure.
- Visit Frequency contrasting controlled with non-controlled patients.
- Testing Frequency
- Referral for diabetes and/or nutritional education
- Numbers of medication
- Appointments not kept
- Whether the target goal is improving, degrading, control lost and if a change in therapy was instituted and if so on what percent of the population it was.
- For patients who have lost control, do they have future appointments, referral for education or referral to a specialist?
- Contrast of quality data points between controlled and uncontrolled, i.e., aspiring prescribed, 10 gm monofilament foot exam, dilated eye exam, annual flu shot, nephropathy screening, smoking cessation.
- Age categories
- Payer class
- Gender
- Socio-economic condition
Diabetes
For an analysis of ethnic disparities, our data for the treatment of diabetes for the past twelve months is as follows:

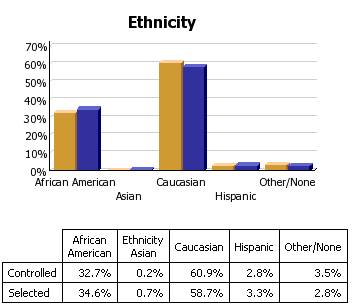
Before the judgment is made that Caucasians receive significantly better healthcare, the bar graph must be described.
- 3783 patients seen by SETMA providers in the past twelve months had diabetes.
- As a percentage of the 3783 patients with diabetes 1,323 were controlled. (For this audit, "controlled" is defined as the patient having had a HgbA1C below 6.5 % for the entire year.) If, as in the case of the National Quality Forum (NQF) Comprehensive Diabetes Measurement Set, "controlled" were defined as below 7% and the measure called for an examination only of the most recent HgbA1C, the percentage of those designated as "controlled" would rise to 59.9%.
- 60.9% of the patients who had diabetes and who were seen in the past twelve months and whose HgbA1c was below 6.5% for the entire year, were Caucasians
- 32.7% of African American treated by SETMA who had diabetes, who were seen in the past twelve months and who had HgbA1C done had a HgbA1C continuously below 6.5%.
- The second classification on this graph is entitled "selected." In the case of the above bar graph, "selected" refers to all patients whose diabetes, at any point in the year, was above 6.5%. There were 2460 of them.
At first glace, it might be assumed that the care of Caucasians was twice as good as that of African Americans. But note that the percentage of "controlled" and "Selected" is not of a subset but a percentage of the same whole. As a percent of the whole, SETMA treats twice as many Caucasians as African Americans. As a percent of those who exhibited continuous control of their diabetes, it is the same proportion of African American as Caucasian. Their treatment judged by process measures or by outcomes measures is identical. The conclusion is that the ethnic distribution of all of SETMA's patients with controlled diabetes is nearly identical to the ethnic distribution of SETMA's patients with uncontrolled diabetes.
Cholesterol (Dyslipidemia)
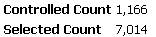
In the case of the treatment of cholesterol (dyslipidemia), the case for the elimination of ethnic disparities of care is not as clear. In the current audit the definition of "controlled" for lipids is a Low Density Lipoprotein (LDL) below 70 mg/dl..
As can be seen by the bar graph below, there is a statistically significant disparity in the care of African Americans with dyslipidemia. Because we have eliminated the financial barriers of access to care for our patients, we recognize that the remaining disparity has to do with life-style, cultural and socio-logical problems. All for which we are working to design solutions. These data represent a total of 8,170 discreet patients with the diagnosis of dyslipidemia.
Approximately 23% of that number are African American and slightly over 70% are Caucasians.
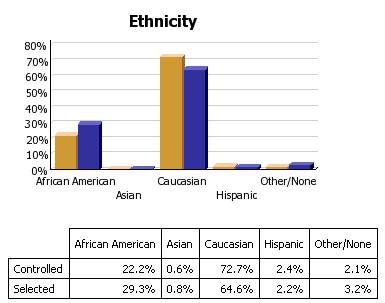
Hypertension
The same explanation applies to hypertension. The goal is to have blood pressure below 130/90 which is defined as "controlled." Again, this audit is displays as "controlled" only those patients whose blood pressure is below 130/90 for the entire year. If we changed the auditing criteria to the last blood pressure being below 130/90, the "controlled" group would rise to over 70%. A total of 8,180 patients where seen in the past 12 months with the diagnosis of hypertension.
Approximately 9,632 discreet patients with hypertension were treated at SETMA in the past twelve months. 6,476 of them had blood pressure readings consistently below 130/90. 3,156 had at least one reading above 130/90.

This disparity is less than that of dyslipidemia but it still exists.
We are designing education programs, dietary management programs and other interventions in an attempt to overcome the remaining disparities in the outcomes of our care of African Americans with these serious health problems.
| 