|
How can healthcare providers design a solution to a complex healthcare problem, particularly when the problem is not generated by a patient's request but by a public-health need. In the former case, the provider simply determines if the request is appropriate or not. In the latter case, no one is in the provider's office requesting a service; a requirement has been established and it is up to the provider, in the midst of many other demands, to remember and to fulfill the requirement. In the case of infectious diseases, requirements have been published for providers to report the occurrence of dozens of conditions.
The problem is that the medical literature is filled with studies showing very low compliance of physicians with reporting infectious diseases to State Health Departments. In Texas, there are 78 infectious diseases which require reporting. The window for reporting compliantly varies from immediately, to one working day, to one week, to ten days, to one month. It is improbable that many healthcare providers know the entire list or the requirement for reporting. The Department of Health wants the report to be triggered by a suspicion and not by a confirmed diagnosis. If the provider waits until the confirmation is made, the opportunity for a public health intervention is lost. A systems solution would be best. The ideal solution would be an electronic medication record (EMR) system in which the reporting action is triggered by the documentation of the diagnoses in the assessment in the EMR.
On April 30, 2011, Dr. Holly made a presentation for a CME program at Texas A&M College of Medicine. The lecturer who followed him was Dr. Edward J. Sherwood, who lectured on "The Ethics of Infectious Disease." Dr. Sherwood distributed a publication of the Texas State Health Department which detailed the 78 reportable conditions. During this presentation, it occurred to Dr. Holly that rather than asking provider to memorize a list of 78 infectious diseases and to organize them into groups according to the time frame in which reporting is required, that the EMR is an ideal means of doing this reporting electronically.
Therefore, SETMA's Information Technology Department was charged with designing a functionality which would:
- Display the reportable conditions for provider review
- Detail the time frame in which each infectious disease should be reported.
- Denote on the display of the reportable conditions the infectious disease which is identified by the provider. This would be done automatically when the diagnosis is documented on the assessment template in the EMR.
- Simultaneous with number three, a telephone message would be sent to SETMA's Care Coordination which would then make the call or send the fax to report the infectious disease. The fact that this had been done will be stored in the EMR in a searchable fashion.
SETMA's Solution to the above
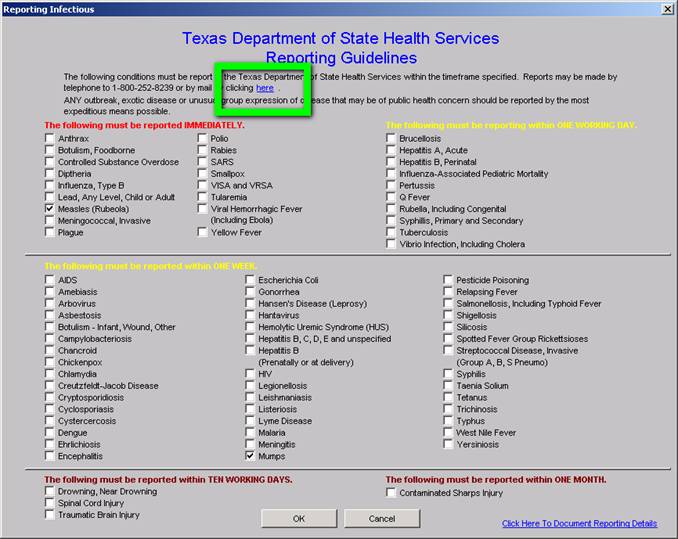
On SETMA's AAA Home template, which is the place where all patient care begins, there is a new button entitled Reportable Conditions. It can be seen below outlined in Green.
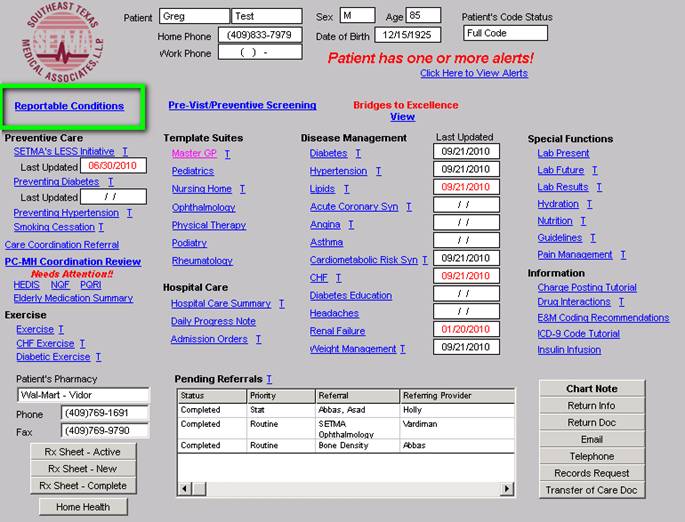
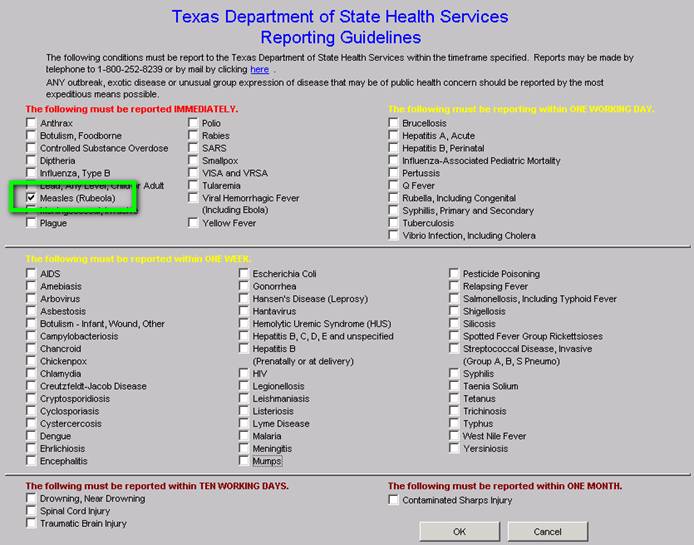
When this button is deployed the following template appears. The template can be used as a review for providers or nurses of what needs to be reported and/or to note that the diagnosed infectious condition, in this case "measles," has been automatically checked as a result of the provider having selected this diagnoses on the assessment template.
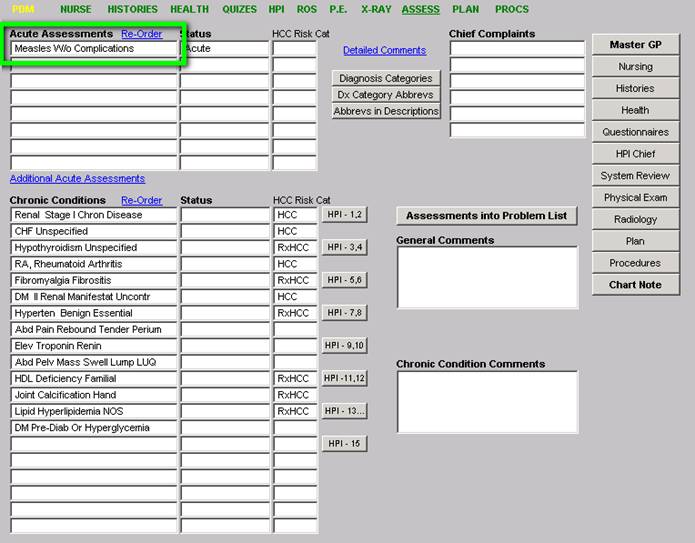
The above checking off of "measles" was noted automatically when the ICD-9 and soon to be ICD-10 code was selected by the provider as is seen below. (Clinicians will amuse themselves with the co-morbidities denoted in this selected "test" patient. It is generally not the case to find measles in patients with diagnoses which are probably from an elderly patient.)
When the infectious disease diagnosis is selected, the system:
- Automatically checks the diagnosed infectious disease on the template where the list of infectious disease is displayed. (see above)
- A telephone message is sent to SETMA's Care Coordination Department.
- The call notification appears in the workflow of the Care Coordination team.
- Once the report is made, a note is added to the patient's chart noting that Health Department notification has been done.
The beauty of this solution is that the provider simply diagnoses a suspected infectious disease and the rest is done without further action by the provider.
The following is the Care Coordination telephone alert which is sent to the nurses in SETMA's Care Coordination Department:
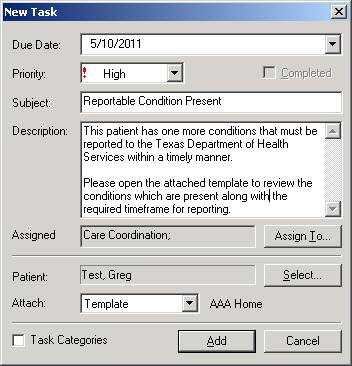
At this point, the process is complete. The entire responsibility of the provider is to make the presumed diagnosis. The remainder is done by a systems protocol which is automatic. We expect this to increase the reporting of infectious disease by SETMA to almost 100% thus improving individual patient care, community care and public health.
Additional Functions
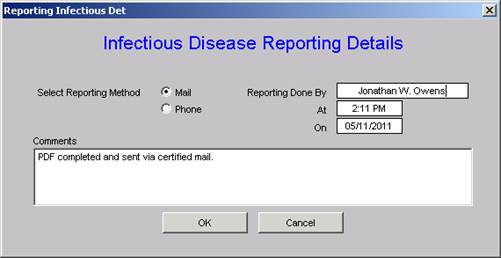
If the provider clicks the link circled below, it will automatically launch a form such that if the provider chooses to report by mail, the form can be printed..
When the Care Coordination department reports the infection, the following allows for the documentation of that report.
Auditing
Quarterly and annually, SETMA will create the following audits:
- How many infectious diseases were documented as having been suspected by providers in the practice? These will be categorized by each of the 78 reportable conditions listed above.
- How many infectious diseases were reported to the appropriate health agency?
- How many of each infectious diseases were reported within the designated time frame?
- If a confirmatory test was performed, what percentage of the report conditions were proved to be present?
This material will be an ongoing quality improvement project by SETMA.
This is a simple but elegant solution to a complex problem which has never been completely solved. It requires no time on the part of the provider. It is measurable and it is sustainable.
Since SETMA designed this solution, several issues have arisen which were unanticipated.
- Does the Department of Health want previously reported incidences of chronic infectious diseases such as hepatitis and HIV to be "re-reported?"
- Does the Department of Health want infectious diseases previously reported in other states reported when the patient moves to Texas?
- Does the state have a way of determining that a chronic infectious disease has been previously reported or not?
- In regard to EMR solutions, the diagnosis of "Coumadin Toxicity" is reported as an "overdose." Obviously, this is not the intent of the desire for public health officials to know the incidence of narcotic or psychotropic drug overdoes. The power of electronics has to be guide so as not to report conditions not intended to be reported.
It is probable that as we proceed, other issues in reporting infectious diseases will arise. The good news is that the above issues have not been considered previously and decisions are being made as to what the answers are. We are all learning and with electronics, we are all participating in improving the care Texans and Americans are receiving.
| 