|
Table of Contents
In 1993, John Patrick set IBM on another course and changed the company's future. Reading his story made me wonder, is it possible for SETMA to set medicine on another course and to change the future. John did not want people to work “collaterally,” side by side, maybe going in the same direction, maybe even having the same goal, but working independently and at best in a cooperative manner; he wanted people to work “collaboratively,” synergistically, leveraging the generative power of a team in creating a new future which they partially envision but which even they could not control.
What can we do today in healthcare which would mirror the changes IBM experienced? How can we change “collaterallists” into “collaborativists”? How can we use the power of electronics, analytics, and informatic principles to energize radical change to create a new future in healthcare? Testing and measurement is a science. In most industries, quality is determined by testing performance. But, in healthcare we are involved in a new kind of “testing.” The tests used to measure the performance of healthcare providers are unique. Therefore, if you are going to measure the quality of care given by healthcare providers:
- If we are going to give a test to healthcare providers, and
- if we are going to give them the test questions before hand, and
- if the test is open-book, and
- if there is no time limit for taking the test;
Why not “cheat?” Look up the answers before the test so providers can know their performance before they get the test results. Don’t wait until an insurer, an ACO, or an agency measures your HEDIS performance. Know your performance by measuring your performance yourself. In fact, know your performance at the time you see a patient. The ultimate “game changer” in healthcare is when the provider knows how he/she is doing in the care of an individual patient, or in the care of a panel or population of patients and then when the provider turns around and shares this information with patients and with the public at large. The game is changed because the motivation to improve is maximized.
There is no cheating!
Of course, ethically there is no “cheating” in this context. Unlike traditional medical-education tests, this test is not measuring what you know; it is measuring what you have access to and it is measuring to what you pay attention. It is measuring how efficiently and excellently you are applying what you know. The test is not measuring what you remember; it is measuring what you are reminded of. If you have Clinical Decision Support (CDS) which remind you of what needs to be done and if you have CDS tools which allow you to measure your own performance at the point of care, you can consistently improve your performance.
In April, 2013, after a three and a half hours presentation of SETMA’s system to eight Medicare Advantage executives, they asked how they could get other providers to perform as well as SETMA. They were told to develop leaders who will help improve the processes and outcomes of care, but that they must recognize also that some times physician leaders use their positions to resist, or to obstruct change rather than to facilitate it. This is not unlike the French Government after World War I.
Determined never to be invaded by Germany again, in the 1930s the French constructed a fixed, defensive fortification between France and Germany called the Maginot Line. The French did not know what General George Patton intuitively knew. In an era of mechanized warfare, fixed fortifications could be and were easily ignored. The enemy went around the Maginot Line. Similarly, when the barrier to healthcare improvement is created by the refusal of healthcare providers to accept new realities and new standards of care, health systems will simply go around them. The intent is to make the obstructing providers irrelevant to the process. The reality is if healthcare providers become fixed fortifications against the future, the process and the system will go around them.
In addition to healthcare providers obstructing the process, there is also the fact that excellent healthcare makes much greater demands of healthcare providers now than ever before. The reality is that many of those demands can be met without active participation by the provider. For instance, one of the most complicated processes healthcare providers are asked to do is to report to the local and state Departments of Health the diagnoses of certain illnesses. In Texas there are seventy eight such illnesses. Just remembering all these conditions is daunting; add to that the need to stop in the middle of a long day to fulfill the reporting requirement is another and perhaps even bigger problem. (For an a complete explanation of SETMA’s solution to infectious disease reporting see Texas State Reportable Infectious Diseases Tutorial.
The lessons of the industrial revolution give us guidance here. Rather than handmade tools and machines made by artisans who were creative geniuses, machines were made by other machines and they were reproduced in mass. Costs went down and quality went up. so the value escalated geometrically. Apply these lessons of standardization, automation and reproducibility to healthcare, we can get to our goals much faster. Henry Ford made a new machine on an assembly line which was nothing more than a standardized, automated method for producing a product which also required human input. If healthcare providers look at every process and outcome in healthcare as a sum of that which can be automated and standardized, and of that which still requires human input, healthcare quality can improve predictably. The cost can be reduced consistently, and provider and patient satisfaction can improve. Some things in healthcare cannot yet be standardized and automated but the satisfaction of receiving the care that can be, will be increased by determining what can be automated and standardized and then by doing so.
The Texas State Health Department’s Reportable Conditions illustrates the standardization and the automation of parts of healthcare processes. Remember, “The more complex a problem is, the more systemic the solution must be.” Today, SETMA providers make a diagnosis, and when that diagnoses is one of the seventy-eight reportable conditions, automatically, the condition is reported to the state with the provider doing nothing more than making the diagnosis. If an important task is not being done either because the provider is resistant to doing it, or because the provider has “too much” to do, automate it.
That question was asked at a conference in Boston in May, 2012. There were many answers, but the question was answered by asking three other questions:
- How important is the task?
- How much time does it take?
- How much energy does it take?
If you were to create a formulae to represent this process, there would be a direct correlation between how many tasks a provider can or will do and how important the tasks are; the more important the tasks, the more tasks a provider will do. There would be an inverse relationship between how much time it takes and how many tasks will be done; the more time it takes, the fewer tasks will be done. There would also be an inverse relationship between how much energy it takes and how many tasks will be done; the more energy it takes, the fewer tasks will be done. The key to getting more done is to determine what is important and only to do that, and then to make the completion of the important tasks require less energy and less time.
Make it easier to do it right than not do it at all! Imitate Henry Ford who automated the manufacturing of automobiles with assembly lines and in so doing made it possible for those who made cars to afford to drive them. There are many aspects of patient care which can be automated. Classically, SETMA has used clinical decision support as reminders to providers, but now we are realizing that many of the tasks which were the object of CDS, actually could and should be automated, requiring no input from the provider. For instance, the value of the flu immunization is not enhanced by it being ordered by a healthcare provider, or by it being given by a registered nurse. And, the process of a flu immunization can be automated.
- When a patient is given an appointment and the system determines that the patient has not had a current flu immunization and the appointment time is in the appropriate time frame to receive the vaccine, the system should order the flu immunization, and send the order to the nurse, to the chart and to charge posting. The provider is not involved which increases the probability that it will be done.
- Additionally, the system should be programmed so that every patient who has not made an appointment in the time frame for a flu immunization should be notified electronically at the beginning of the flu-immunization season that they need to have a flu shot and toward the end of the immunization season, the system should check again to see who has not had the shot.
This principle can be expanded to all chronic conditions for which the patient is being treated and/or for all screening and preventive care the patient requires. In the future, all healthcare process will be evaluated for:
- That which can and should be automated, all based on evidence-based medicine
- That which requires human input based on patient-centered care
This will give the healthcare provider more time to focus on the patient while fulfilling the processes (care) which we believe will improve the health (outcomes) and which will decrease the cost of excellent care. Automation of care can help healthcare providers fulfill the “triple aim.”
In June, 2013, the American Medical News published an article entitled, “Serious work put into making primary care fun again.” With an anticipated serious shortage of primary care physicians over the next twenty years, the article addressed how to improve the lot of primary care providers, stating in part: “Amid alarming rates of physician burnout, hundreds of clinics nationwide are redesigning their practices with a goal in mind beyond improving the quality of care. They are aiming to make life as a primary care doctor enjoyable once more. Twenty-three of these clinics...describe practice innovations that can ease the chaos, administrative overload, miscommunication and computerized busy work that too often characterize primary care. These clinics found that:
- Planning visits ahead of time,
- Delegating more tasks to nurses and medical assistants,
- Holding daily meetings and
- Using standing orders for recurring items
not only improves patient satisfaction but also creates happier doctors.” The study also found, “Physician satisfaction is an essential ingredient in transforming the delivery of medical care...” All medical care, and especially primary care, is incredibly complex, creative work that requires willing, engaged participants and strong support to be successful. The study said, “....We use silly words like ‘joy’' and ‘love’ and ‘hope’ because that's what we need. We don't need more rules or checklists or regulations.”
Reviewing the recommendations from these clinics, SETMA is already doing all of the things they recommend but SETMA believes the processes of care can be improved even more. And, It is obvious that the improvements we discussed will also improve the professional satisfaction of primary healthcare providers and that those improvements will decrease the stress upon primary care providers.
Over the next two years, SETMA will examine the care given in our ambulatory clinics In creating The Automated Team, the first step will be to automate the care of diabetes as much as is possible. The effort to improve the care of patients with diabetes involves the fulfillment of “process measures,” which are tasks, such as:
- Has the patient had a hemoglobin A1c within the past three months?
- Has the patient has a urinalysis in the past year?
- Has the patient had a dilated eye examination in the past year? The complexity of this question is that if a referral is automatically created for a dilated eye examination, and the patient is seen again before that examination has been completed, can the system know that and not create a redundant referral? The answer is, “Yes,” Secondly, if the automated referral is completed and the patient is seen after the examination has been done but the report is not found in the record, can the system create instructions for the report to be obtained? The answer again is, “Yes,” Any process can be analyzed beyond a first or second or third step to make the automation reliable and beneficial for patient care.
- Has the patient had an examination of the feet in the past year including a test of feeling in the feet?
- Has the patient had a test for protein in the urine in the past year?
- Has the patient had a flu immunization in the past year?
- Has the patient had a cholesterol test in the past year?
- Is the patient on a statin drug?
- Is the patient on aspirin?
- If the patient has protein in the urine, is the patient on an ACE Inhibitor or an ARB (blood pressure medicines that prevents protein in the urine or helps reduce it if it has already occurred)?
This effort also involves “outcomes measures,” which means to evaluate whether diabetes care meets established goals, such as:
- Is the patient’s hemoglobin A1c below 7.0%?
- Is the patient’s “bad cholesterol,” the LDL, below 70?
- Is the patient’s blood pressure controlled below 130/90?
- If the patient is overweight or obese, is he/she losing weight?
- Is the patient devoid of complications and if he or she is not, has the worsening of the complication been arrested?
This effort also involves patient “lifestyle measures,” such as:
- Is the patient exercising regularly and has the patient been given an exercise prescription in the past 90 days?
- Has the patient been asked about smoking or exposure to tobacco smoke and if either is true has the patient been given help in stopping smoking?
- Has the patient been given instructions on how to lose weight, how to read processed food labels and is the patient following a diet?
- Has the patient been to diabetes education classes in the past twelve months?
- Is the patient monitoring their own blood sugar at home?
- Does the patient keep a blood sugar and a blood pressure log?
Most of these tasks can be “automated, “which means that they can be ordered before the patient comes to the clinic. In the design of The Automated Team functions, when the patient makes an appointment, the EMR automatically searches the patient’s record and creates orders for referrals, procedures and tests. At the time of the visit, in The Automated Team functions, the following documents are also created:
- A summary of the patient’s needed care for the nurse who will see the patient.
- A summary of patient needs for improvement of care and for removing as much stress as possible from the provider, such as alerting the provider that the blood pressure, or the blood sugar, or the cholesterol, or other outcomes measures are not to goal.
- A summary of tests, procedures or referrals which have been initiated for the patient. This summary will explain what has been ordered, where and when the care will be competed and an explanation of why the care has been ordered and the benefit of the care to the patient.
These steps will improve the quality of care for the patient and the quality of life for the provider. A great deal of stress will be taken off the provider who will have more time to spend with the patient giving attention to the patient’s interests rather than spending time fulfilling important but easily automated tasks. It is possible that this process will reduce the work load of the healthcare provider by 30% or more. If it does, it will be transformative to primary care by giving the provider the capacity to fulfill quality metrics while spending more time and attention on the patient.
The Vision
As we learn more about how to improve our health and as we are able to change the future of our health more, excellence in healthcare increasingly is dependent upon two things: a team approach and the automation of those standardized tasks, which while they are critical to excellent care, can be completed without requiring the time and attention of team members. This gives the team more time to interact with one another personally. This standardization and automation of care brings us one step closer to the ultimate promise of electronic patient management which is the ultimate goal of electronic patient records. The Automated Team is the logical extension of clinical decision support.
The Team
The majority of healthcare is delivered and received in the ambulatory setting in a clinician’s office. While the healthcare team is much boarder, in the ambulatory setting, the principle members of the team are the patient, the nursing staff and the healthcare provider. Ultimately, while the standardization and automation of this team’s functions will spread across all areas of care, Southeast Texas Medical Associates’ efforts begin with diabetes. Each member of the team - patient, nurse, and provider -- contribute to the excellence of ambulatory care for diabetes.
The Plan
When a patient who has diabetes makes an appointment, based on evidenced-based medicine and national standards of care, the electronic record will immediately search the patient’s entire medical record to determine what tests, procedures, consultations or interventions are required and which have not been performed. Each of these interventions will be directed at the prevention of the complications of diabetes and/or at the improvement of the care of the patient with diabetes. Because diabetes is a progressive disease, excellence of care at one point in time may not reflect excellence of care at another time, thus the reason why the “automated team” needs an updated, current and complete plan of care and treatment plan at each visit.
The Automation
When the patient presents for their appointment, three documents will have been prepared:
- For the nurse, a document will have been prepared which lets the nurse know what elements of his/her contribution to the team’s effort are not up to date and need to be addressed, such as The LESS Initiative, the 10-gram monofilament sensory examination, immunizations, medication reconciliation, etc.
- For the patient, a patient engagement and activation document will have been prepared which tells the patient what tests, procedures or referrals have been scheduled. An explanation will be provided to the patient as to why he/she is being asked to have these tests, procedures, or appointments. As stated above, all interventions will be directed toward the improvement of the patient’s care and the avoidance of the complications of diabetes. With this document, the patient will know what his/her responsibility is to support the efforts of the team.
- For the provider, a document will have been prepared which explains the information which has been given to the nurse and the patient. The provider will be alerted to whether or not the patient has been treated to goal for diabetes and if they are not, the provider will be encouraged to change medication, life-styles, education, etc., in order to achieve control.
The Team’s Activation - True Patient-Centered Care
Each team member will have access to the documents given to other members of the team. Each team member will know what is expected of the team and each team member will know the goals are for the entire team. Because the team will be spending less time on the tasks of ordering and scheduling tests, procedures and referrals, there will be more time for the building of relationships and for the engagement and activation of each member of the team.
Over time, SETMA will build the Automated Team functions for all chronic diseases, such as hypertension, congestive heart failure, chronic renal disease, cardiometabolic risk syndrome. The Automated Team functions will also be built for the fulfillment of HEDIS measures, ACO quality metrics,, Medicare Advantage STARS quality metrics, and for the over 300 quality metrics SETMA currently tracks, audits, analyzes and publicly reports of provider performance by provider name. SETMA hopes to have all of the Automated Team functions for all of the chronic conditions we treat built over the next twelve months.
When a patient makes an appointment, the computer automatically and independently:
- Searches the patient’s record for all chronic conditions for which the patient is being treated.
- Creates orders for procedures and tests and referrals for appointments with other providers
- Creates a patient engagement and activation document, a nurse’s responsibility document and recommendations to healthcare document
This will leave more time for the provider to listen to the patient’s healthcare concerns and desires, to modify the patient’s plan of care and treatment plan to improve outcomes and to make certain that the grasps the “baton” through which the patent will accept responsibility for their care.
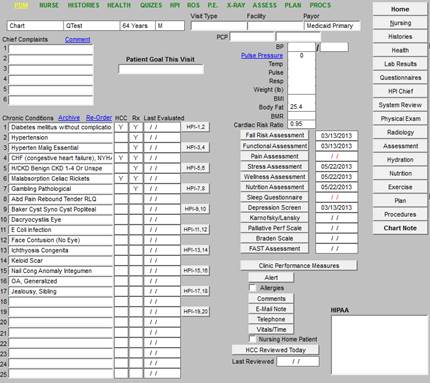
The following is the Master Ambulatory Template in SETMA’s EMR where the patient’s chronic conditions are recorded. This is he list which is search in order to fulfill The Automated Team functions. Currently, the Automated Team functions are only active for diabetes. Because the below is a “sample” chart, the chronic conditions have been placed randomly. In a real patient’s chart, it is important routinely to do “chronic problem list reconciliation” in order to maximize efficiency and effectiveness of patient care.
Note: If a patient has a referral created for a Dilated Eye Examination, and is seen again before the test is completed, the system will recognize that the referral has been made and a second referral will not be created. If after six months, the patient is seen and there is no documentation that the referral results have been returned, the system will generate a note to medical records asking them to inquire about the results.
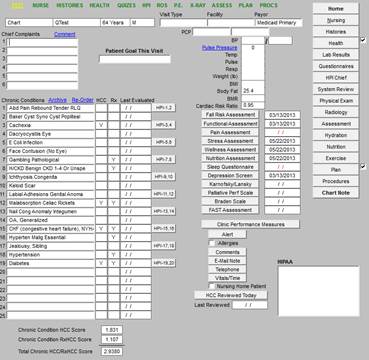
One of the six functions of “chronic problem list reconciliation” is the “re-ordering” of the list. The following is a link to the tutorial for how SETMA re-orders the “Chronic Problem list.” Problem List Reconciliation: The Tools Required to Facilitate the Maintenance of a Current, Valid and Complete Chronic Problem List in an EMR. Because of the tool we have built this takes only a few seconds and the following is the result.
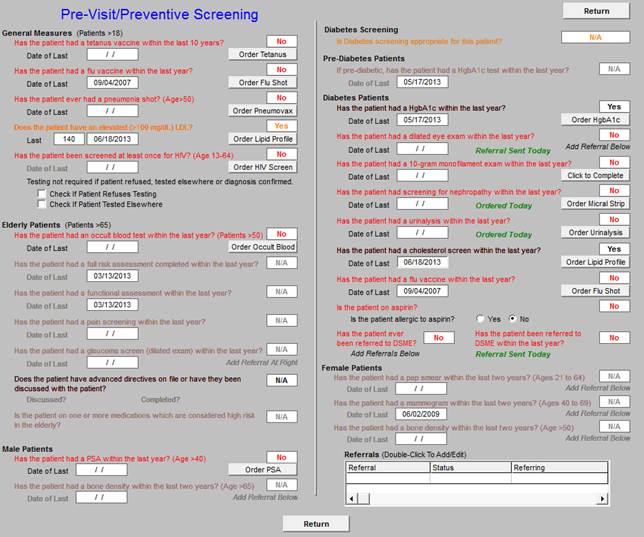
Every ambulatory visit at SETMA starts with the Pre-Visit/Preventive Screening template which is seen below. The illustration below shows the template after it has been deployed, which means that the notations created by The Automated Team functions are already present on the template.
The legend for this template is that all elements in black apply to the patient and have been done. All elements in grey, do not apply to the patient and all items which apply to the patient and which have not been done appear in red. When the template is opened, all elements of diabetes are automatically searched by the computer and the elements of diabetes care which have not been done are automatically completed. The completed items are noted in green on this template. Eventually, all items on this template will be automated but SETMA has started with diabetes.
Once any non-automated measures have been dealt with, the nurse and/or provider will click the button entitled “return.” At that time, three documents will be automatically created. They are discussed and illustrated below. There is a document for the nurse, for the patient and for the healthcare provider. All members of the ambulatory healthcare team will receive all information given to the other members of the team:
- The information given to the nurse will also appear on the document prepared for the patient and for the provider.
- The information given to the patient will also appear on the document provided for the nurse and the provider.
- The information given to the provider will also appear on the document provided to the patient and the nurse.
We believe that when complete, the Automated Team functions will free up 25-35% of the healthcare providers’ time, allowing all quality issues to be completed successfully and allowing the healthcare provider to spend more time with the patient.
There is one major question which we hope to answer over the next three years. SETMA providers currently meet the standards for NCQA Diabetes Recognition, NCQA Tier III and AAHC Patient-Centered Medical Home standards, and we have submitted the completed application for Cardiac/Stroke Recognition. We expect the Automated Team function to improve our already excellent performance with less effort and less time required by the provider.
The question is, “Will the Automated Team functions, which should have all SETMA providers consistently fulfilling all quality metrics and patient information materials, improve outcomes of care?
We know what our outcomes performance has been with clinical decision support (CDS) tools, with this expansion of the CDS tools into the Automated Team functions, will our performance and patient outcomes continue to improve? We expect so, but only time will tell.
While decreasing stress on providers and freeing up more time for patient interaction are important goals of The Automated Team, the greatest promise for improving outcomes come frm patient engagement and activation. To facilitate patient engagement and activation, the patient will be informed by staff teaching and by a document as to the tests, procedures and referrals which have been initiated by automation.
The following are the potential orders for patients with diabetes. In the patient’s document, the explanations and rationale for procedures, tests and referrals will be automatically selected from the following options. (see sample Patient Engagement and Activation document below).
All patients with diabetes need an annual dilated examination performed by an ophthalmologist. The most common cause of blindness in the United States is uncontrolled diabetes. The annual examination allows complications to be recognized early when treatment can be undertaken to preserve your sight. Note: If a referral has been made for you and you have had a dilated eye examination in the past six months, please let your provider and/or your nurse know.
- 10-gram Monofilament Examination
The most common cause of non-traumatic amputations of a limb in the United States is uncontrolled diabetes. The first step toward losing a limb is the loss of sensation in the lower extremity. It is very important that every person with diabetes has an examination of sensory perception in the lower extremity. This is done with a non-invasive examination with a 10-gram monofilament. This examination will be completed in the office by your nurse. It is an important part of the care of your diabetes.
All patients with diabetes should have their feet examined at each visit. In addition to the sensory examination, the feet are examined for ulcers, wounds, infections or other skin abnormalities. Patients with diabetes should not trim their own toenails, go barefoot or subject yourself to potential foot or toe injuries. If you have decreased or absence sensory perception you should be seen by a podiatrist annually. The sensory examination and proper foot care are the first steps to preserving your limbs./.
- Diabetes Self Management Education (DSME) and/or Medical Nutrition Therapy (MNT)
Dr. Joslin, the founder of the Diabetes Center of Excellence, said, “The person who knows the most about diabetes will live the longest.” If you have not attended DSME classes and if you have not attended MNT classes, you must attend an initial complete course. If you have been through the complete courses, you should attend an annual refresher course. The dietician and/or Certified Diabetes Educator can help you with dietary information about diabetes, high blood pressure, cholesterol, weight reduction and many other conditions. SETMA’s diabetes education program is certified by the American Diabetes Association.
This blood test allows you to know what your average blood sugar has been over the past three months. If your HbA1c is higher than 7.0% you are a higher risk for diabetes complications. Because you have not had a HbA1c in the past three months, an order has been created for you to have a test today. You do not have to be fasting for this test. If you HbA1c is above 7.0%, ask your healthcare provider what you can and should do to control your blood glucose.
Diabetes is a significant risk factor for cardiovascular disease, as are certain types of cholesterol abnormality. With the values of this examination, your Cardiovascular Metabolic Risk Assessment and your Framingham Cardiovascular Risk Score can be calculated. These assessment will allow your care to be managed appropriately and with SETMA’s unique “Framingham Cardiovascular Risk ‘What if Scenario,’” you can know how a the life-style and health changes you make will make a difference in your future health.
Because your urine is produced by the kidneys, an examination of your urine will tell your healthcare provider a great deal about the health of your kidneys. Annually, all patients with diabetes should have their urine examined for infection, protein, glucose and other abnormalities.
- Micral Strip or Albumin/Creating Ratio
The most common cause of kidney failure is uncontrolled diabetes. Beyond the UA, an annual test for renal disease and/or for abnormal protein in the urine enables you and your provider to anticipate and hopefully avoid kidney problems. The micral strip and the albumin/creatinine ratio are simple non-invasive means of accessing your kidney function and the results of these tests will help you healthcare provider calculate your Estimate Glomerular Filtration Rate (eGFR) which is an even more sensitive measure of your kidney function.
If you have not had, or if you have refused to have an annual flu shot, an every ten-year Tdap (Tetanus, Diphtheria, Acellular Pertussus), or an every ten-year pneumonia vaccine (Pneumonvax), you should agree to these preventive measures. The increased infectious risk for patients with diabetes makes these immunizations increasingly important to maintain. Unless you are allergic to eggs, there is no medical reason for you not to have your immunizations and it is an important part of your care. Note: There is some evidence for an annual flu shot to have some cardiovascular risk benefit.
If you are not taking a low-dose aspirin and you are not allergic to aspirin, you should start taking an 81 mg aspiring daily. Discuss this with your healthcare provider. If you are allergic to aspirin you should not take it. If you take large doses of fish oil, Coumadin, Pradaxa or Plavix, you should discuss aspirin with your healthcare provider before taking it.
If you are not excising routinely, you must know that nothing is more important to your health than routine exercise (walking, swimming) for 30-45 minutes four days or more a week. At SETMA you will have received a copy of your personalized exercise prescription in the LESS Initiative. Start slowly - how fast you start is not as important as how consistently you exercise - and work within your capacity.
If you smoke, or if you are exposed to tobacco smoke, your health is at significantly higher risk and you should asks your healthcare provider for help in stopping. No patient with diabetes should add to their heart disease risk by smoking.
If you are overweight or obese, you should take stapes (exercise and dietary) to lose weight. Ask you provider for help. SETMA’s nutritionist can give you counsel about how to change your life styles to improve your BMI and BMR (these terms are defined in your LESS Initiative.
It takes a team to treat diabetes; without the activated, engaged participation of each team member, the entire team will fail. Below you will see the information given to your other team members. The more the entire team knows about the responsibilities of the other team members, and the more engaged each team member is with other team members, the more successfully the automated team's efforts will be.
As more conditions are brought on line for The Activated Team functions, this list will grow and the documents shown below will expand.

SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Patient Engagement and Activation Information
Patient ChartQTest
DOB 03/01/1949
Encounter 06/25/2013 8:00 AM
The Automated Team - Introduction
The Vision
As we learn more about how to improve our health and as we are able to change the future of our health more, excellence in healthcare increasingly is dependent upon two things: a team approach and the automation of those standardized tasks, which while they are critical to excellent care, can be completed without requiring the time and attention of team members. This gives the team more time to interact with one another personally. This standardization and automation of care brings us one step closer to the ultimate promise of electronic patient management which is the ultimate goal of electronic patient records.
The Team
The majority of healthcare is delivered and received in the ambulatory setting in a clinician's office. While the healthcare team is much boarder, in the ambulatory setting, the principle members of the team are the patient, the nursing staff and the healthcare provider. Ultimately, while the standardization and automation of this teams functions will spread across all areas of care, Southeast Texas Medical Associates efforts begin with diabetes. Each member of the team patient, nurse, provider -- contribute to the excellence of ambulatory care for diabetes.
The Plan
When a patient who has diabetes makes an appointment, based on evidenced-based medicine and national standards of care, the electronic record will immediately search the patient's entire medical record to determine what tests, procedures, consultations or interventions are required and which have not been performed. Each of these interventions will be directed at the prevention of the complications of diabetes and/or at the improvement of the care of the patient with diabetes. Because diabetes is a progressive disease, excellence of care at one point in time may not reflect excellence of care at another time, thus the reason why the “automated team” needs an updated, current and complete plan of care and treatment plan at each visit.
The Automation
When the patient presents for their appointment, three documents will have been prepared:
- For the nurse, a document will have been prepared which lets the nurse know what elements of his/her contribution to the teams effort are not up to date and need to be addressed, such as The LESS Initiative, the 10-gram monofilament sensory examination, immunizations, medication reconciliation, etc.
- For the patient, a document will have been prepared which tells the patient what tests, procedures or referrals have been scheduled. An explanation will be provided to the patient as to why he/she is being asked to have these tests, procedures, or appointments. As stated above, all interventions will be directed toward the improvement of the patients care and the avoidance of the complications of diabetes. With this document, the patient will know what his/her responsibility is to support the efforts of the team.
- For the provider, a document will have been prepared which explains the information which has been given to the nurse and the patient. The provider will be alerted to whether or not the patient has been treated to goal for diabetes and if they are not, the provider will be encouraged to change medication, life-styles, education, etc., in order to achieve control.
The Teams Activation - True Patient-Centered Care
Each team member will have access to the documents given to other members of the team. Each team member will know what is expected of the team and each team member will know the goals are for the entire team. Because the team will be spending less time on the tasks of ordering and scheduling tests, procedures and referrals, there will be more time for the building of relationships and for the engagement and activation of each member of the team.
The following tests, procedures and referrals have been made for you. The reasons for each of these orders are listed below. You will be contacted for the time and place for any referrals made.
Dilated Eye Examination
All patients with diabetes need an annual dilated examination performed by an ophthalmologist. The most common cause of blindness in the United States is uncontrolled diabetes. The annual examination allows complications to be recognized early when treatment can be undertaken to preserve your sight. Note: If a referral has been made for you and you have had a dilated eye examination in the past six months, please let your provider and/or your nurse know.
10-Gram Monofilament Examination
The most common cause of non-traumatic amputations of a limb in the United States is uncontrolled diabetes. The first step toward losing a limb is the loss of sensation in the lower extremity. It is very important that every person with diabetes has an examination of sensory perception in the lower extremity. This is done with a non-invasive examination with a 10-gram monofilament. This examination will be completed in the office by your nurse. It is an important part of the care of your diabetes.
Podiatry
All patients with diabetes should have their feet examined at each visit. In addition to the sensory examination, the feet are examined for ulcers, wounds, infections or other skin abnormalities. Patients with diabetes should not trim their own toenails, go barefoot or subject yourself to potential foot or toe injuries. If you have decreased or absence sensory perception you should be seen by a podiatrist annually. The sensory examination and proper foot care are the first steps to preserving your limbs./.
Diabetes Self Management Education (DSME) and/or Medical Nutrition Therapy (MNT)
Dr. Joslin, the founder of the Diabetes Center of Excellence, said, “The person who knows the most about diabetes will live the longest.” If you have not attended DSME classes and if you have not attended MNT classes, you must attend an initial complete course. If you have been through the complete courses, you should attend an annual refresher course. The dietician and/or Certified Diabetes Educator can help you with dietary information about diabetes, high blood pressure, cholesterol, weight reduction and many other conditions. SETMAs diabetes education program is certified by the American Diabetes Association.
Urinalysis (UA)
Because your urine is produced by the kidneys, an examination of your urine will tell your healthcare provider a great deal about the health of your kidneys. Annually, all patients with diabetes should have their urine examined for infection, protein, glucose and other abnormalities.
Micral Strip or Albumin/Creating Ratio
The most common cause of kidney failure is uncontrolled diabetes. Beyond the UA, an annual test for renal disease and/or for abnormal protein in the urine enables you and your provider to anticipate and hopefully avoid kidney problems. The micral strip and the albumin/creatinine ratio are simple non-invasive means of accessing your kidney function and the results of these tests will help you healthcare provider calculate your Estimate Glomerular Filtration Rate (eGFR) which is an even more sensitive measure of your kidney function.
Immunizations
If you have not had, or if you have refused to have an annual flu shot, an every ten-year Tdap (Tetanus, Diphtheria, Acellular Pertussus), or an every ten-year pneumonia vaccine (Pneumonvax), you should agree to these preventive measures. The increased infectious risk for patients with diabetes makes these immunizations increasingly important to maintain. Unless you are allergic to eggs, there is no medical reason for you not to have your immunizations and it is an important part of your care. Note: There is some evidence for an annual flu shot to have some cardiovascular risk benefit.
Aspirin
If you are not taking a low-dose aspirin and you are not allergic to aspirin, you should start taking an 81 mg aspiring daily. Discuss this with your healthcare provider. If you are allergic to aspirin you should not take it. If you take large doses of fish oil, Coumadin, Pradaxa or Plavix, you should discuss aspirin with your healthcare provider before taking it.
Exercise
If you are not excising routinely, you must know that nothing is more important to your health than routine exercise (walking, swimming) for 30-45 minutes four days or more a week. At SETMA you will have received a copy of your personalized exercise prescription in the LESS Initiative. Start slowly how fast you start is not as important as how consistently you exercise and work within your capacity.
Tobacco
If you smoke, or if you are exposed to tobacco smoke, your health is at significantly higher risk and you should asks your healthcare provider for help in stopping. No patient with diabetes should add to their heart disease risk by smoking.
Excess Weight
If you are overweight or obese, you should take stapes (exercise and dietary) to lose weight. Ask you provider for help. SETMAs nutritionist can give you counsel about how to change your life styles to improve your BMI and BMR (these terms are defined in your LESS Initiative.
Conclusion
It takes a team to treat diabetes; without the activated, engaged participation of each team member, the entire team will fail. Below you will see the information given to your other team members. The more the entire team knows about the responsibilities of the other team members, and the more engaged each team member is with other team members, the more successfully the automated team's efforts will be.
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Nursing Responsibilities
The following need to be completed for this patient.
10-gram Monofilament Foot Exam
Evaluation of Renal Status
Cardiometabolic Risk Syndrome Assessment
Framingham Risk Assessment
Discuss Aspirin Use
Discuss Flu Vaccination
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Provider Responsibilities
The patient's most recent lab values are as follows.
| HbA1c | 6.5% | 05/17/2013 |
| Cholesterol | 215 mg/dL | 06/18/2013 |
| LDLC | 140 mg/dL | 06/18/2013 |
| Triglycerides | 99 mg/dL | 06/18/2013 |
| HDL | 55 mg/dL | 06/18/2013 |
The patient's lipids are not treated to goal. Take measures to move the patient toward goal of LDL < 70 mg/dL.
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Patient Chart QTest
DOB 03/01/1949
Encounter 06/25/2013 8:00 AM
The Automated Team - Introduction
The Vision
As we learn more about how to improve our health and as we are able to change the future of our health more, excellence in healthcare increasingly is dependent upon two things: a team approach and the automation of those standardized tasks, which while they are critical to excellent care, can be completed without requiring the time and attention of team members. This gives the team more time to interact with one another personally. This standardization and automation of care brings us one step closer to the ultimate promise of electronic patient management which is the ultimate goal of electronic patient records.
The Team
The majority of healthcare is delivered and received in the ambulatory setting in a clinician's office. While the healthcare team is much boarder, in the ambulatory setting, the principle members of the team are the patient, the nursing staff and the healthcare provider. Ultimately, while the standardization and automation of this teams functions will spread across all areas of care, Southeast Texas Medical Associates efforts begin with diabetes. Each member of the team patient, nurse, provider -- contribute to the excellence of ambulatory care for diabetes.
The Plan
When a patient who has diabetes makes an appointment, based on evidenced-based medicine and national standards of care, the electronic record will immediately search the patient's entire medical record to determine what tests, procedures, consultations or interventions are required and which have not been performed. Each of these interventions will be directed at the prevention of the complications of diabetes and/or at the improvement of the care of the patient with diabetes. Because diabetes is a progressive disease, excellence of care at one point in time may not reflect excellence of care at another time, thus the reason why the “automated team” needs an updated, current and complete plan of care and treatment plan at each visit.
The Automation
When the patient presents for their appointment, three documents will have been prepared:
- For the nurse, a document will have been prepared which lets the nurse know what elements of his/her contribution to the teams effort are not up to date and need to be addressed, such as The LESS Initiative, the 10-gram monofilament sensory examination, immunizations, medication reconciliation, etc.
- For the patient, a document will have been prepared which tells the patient what tests, procedures or referrals have been scheduled. An explanation will be provided to the patient as to why he/she is being asked to have these tests, procedures, or appointments. As stated above, all interventions will be directed toward the improvement of the patients care and the avoidance of the complications of diabetes. With this document, the patient will know what his/her responsibility is to support the efforts of the team.
- For the provider, a document will have been prepared which explains the information which has been given to the nurse and the patient. The provider will be alerted to whether or not the patient has been treated to goal for diabetes and if they are not, the provider will be encouraged to change medication, life-styles, education, etc., in order to achieve control.
The Teams Activation - True Patient-Centered Care
Each team member will have access to the documents given to other members of the team. Each team member will know what is expected of the team and each team member will know the goals are for the entire team. Because the team will be spending less time on the tasks of ordering and scheduling tests, procedures and referrals, there will be more time for the building of relationships and for the engagement and activation of each member of the team.
The following need to be completed for this patient.
10-gram Monofilament Foot Exam
Evaluation of Renal Status
Cardiometabolic Risk Syndrome Assessment
Framingham Risk Assessment
Discuss Aspirin Use
Discuss Flu Vaccination
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
Conclusion
It takes a team to treat diabetes; without the activated, engaged participation of each team member, the entire team will fail. Below you will see the information given to your other team members. The more the entire team knows about the responsibilities of the other team members, and the more engaged each team member is with other team members, the more successfully the automated team's efforts will be.
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Patient Engagement and Activation Information
Automated Orders for Chart QTest
The following tests, procedures and referrals have been made for you. The reasons for each of them have been listed below. You will be contacted for the time and place for any referrals made.
Dilated Eye Examination
All patients with diabetes need an annual dilated examination performed by an ophthalmologist. The most common cause of blindness in the United States is uncontrolled diabetes. The annual examination allows complications to be recognized early when treatment can be undertaken to preserve your sight. Note: If a referral has been made for you and you have had a dilated eye examination in the past six months, please let your provider and/or your nurse know.
10-Gram Monofilament Examination
The most common cause of non-traumatic amputations of a limb in the United States is uncontrolled diabetes. The first step toward losing a limb is the loss of sensation in the lower extremity. It is very important that every person with diabetes has an examination of sensory perception in the lower extremity. This is done with a non-invasive examination with a 10-gram monofilament. This examination will be completed in the office by your nurse. It is an important part of the care of your diabetes.
Podiatry
All patients with diabetes should have their feet examined at each visit. In addition to the sensory examination, the feet are examined for ulcers, wounds, infections or other skin abnormalities. Patients with diabetes should not trim their own toenails, go barefoot or subject yourself to potential foot or toe injuries. If you have decreased or absence sensory perception you should be seen by a podiatrist annually. The sensory examination and proper foot care are the first steps to preserving your limbs./.
Diabetes Self Management Education (DSME) and/or Medical Nutrition Therapy (MNT)
Dr. Joslin, the founder of the Diabetes Center of Excellence, said, “The person who knows the most about diabetes will live the longest.” If you have not attended DSME classes and if you have not attended MNT classes, you must attend an initial complete course. If you have been through the complete courses, you should attend an annual refresher course. The dietician and/or Certified Diabetes Educator can help you with dietary information about diabetes, high blood pressure, cholesterol, weight reduction and many other conditions. SETMAs diabetes education program is certified by the American Diabetes Association.
Urinalysis (UA)
Because your urine is produced by the kidneys, an examination of your urine will tell your healthcare provider a great deal about the health of your kidneys. Annually, all patients with diabetes should have their urine examined for infection, protein, glucose and other abnormalities.
Micral Strip or Albumin/Creating Ratio
The most common cause of kidney failure is uncontrolled diabetes. Beyond the UA, an annual test for renal disease and/or for abnormal protein in the urine enables you and your provider to anticipate and hopefully avoid kidney problems. The micral strip and the albumin/creatinine ratio are simple non-invasive means of accessing your kidney function and the results of these tests will help you healthcare provider calculate your Estimate Glomerular Filtration Rate (eGFR) which is an even more sensitive measure of your kidney function.
Immunizations
If you have not had, or if you have refused to have an annual flu shot, an every ten-year Tdap (Tetanus, Diphtheria, Acellular Pertussus), or an every ten-year pneumonia vaccine (Pneumonvax), you should agree to these preventive measures. The increased infectious risk for patients with diabetes makes these immunizations increasingly important to maintain. Unless you are allergic to eggs, there is no medical reason for you not to have your immunizations and it is an important part of your care. Note: There is some evidence for an annual flu shot to have some cardiovascular risk benefit.
Aspirin
If you are not taking a low-dose aspirin and you are not allergic to aspirin, you should start taking an 81 mg aspiring daily. Discuss this with your healthcare provider. If you are allergic to aspirin you should not take it. If you take large doses of fish oil, Coumadin, Pradaxa or Plavix, you should discuss aspirin with your healthcare provider before taking it.
Exercise
If you are not excising routinely, you must know that nothing is more important to your health than routine exercise (walking, swimming) for 30-45 minutes four days or more a week. At SETMA you will have received a copy of your personalized exercise prescription in the LESS Initiative. Start slowly how fast you start is not as important as how consistently you exercise and work within your capacity.
Tobacco
If you smoke, or if you are exposed to tobacco smoke, your health is at significantly higher risk and you should asks your healthcare provider for help in stopping. No patient with diabetes should add to their heart disease risk by smoking.
Excess Weight
If you are overweight or obese, you should take stapes (exercise and dietary) to lose weight. Ask you provider for help. SETMAs nutritionist can give you counsel about how to change your life styles to improve your BMI and BMR (these terms are defined in your LESS Initiative.
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
The patient's most recent lab values are as follows.
| HbA1c | 6.5% | 05/17/2013 |
| Cholesterol | 215 mg/dL | 06/18/2013 |
| LDLC | 140 mg/dL | 06/18/2013 |
| Triglycerides | 99 mg/dL | 06/18/2013 |
| HDL | 55 mg/dL | 06/18/2013 |
The patient's lipids are not treated to goal. Take measures to move the patient toward goal of LDL < 70 mg/dL.
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Provider Responsibilities
Patient ChartQTest
DOB 03/01/1949
Encounter 06/25/2013 8:00 AM
The Automated Team - Introduction
The Vision
As we learn more about how to improve our health and as we are able to change the future of our health more, excellence in healthcare increasingly is dependent upon two things: a team approach and the automation of those standardized tasks, which while they are critical to excellent care, can be completed without requiring the time and attention of team members. This gives the team more time to interact with one another personally. This standardization and automation of care brings us one step closer to the ultimate promise of electronic patient management which is the ultimate goal of electronic patient records.
The Team
The majority of healthcare is delivered and received in the ambulatory setting in a clinician's office. While the healthcare team is much boarder, in the ambulatory setting, the principle members of the team are the patient, the nursing staff and the healthcare provider. Ultimately, while the standardization and automation of this teams functions will spread across all areas of care, Southeast Texas Medical Associates efforts begin with diabetes. Each member of the team patient, nurse, provider -- contribute to the excellence of ambulatory care for diabetes.
The Plan
When a patient who has diabetes makes an appointment, based on evidenced-based medicine and national standards of care, the electronic record will immediately search the patient's entire medical record to determine what tests, procedures, consultations or interventions are required and which have not been performed. Each of these interventions will be directed at the prevention of the complications of diabetes and/or at the improvement of the care of the patient with diabetes. Because diabetes is a progressive disease, excellence of care at one point in time may not reflect excellence of care at another time, thus the reason why the “automated team” needs an updated, current and complete plan of care and treatment plan at each visit.
The Automation
When the patient presents for their appointment, three documents will have been prepared:
- For the nurse, a document will have been prepared which lets the nurse know what elements of his/her contribution to the teams effort are not up to date and need to be addressed, such as The LESS Initiative, the 10-gram monofilament sensory examination, immunizations, medication reconciliation, etc.
- For the patient, a document will have been prepared which tells the patient what tests, procedures or referrals have been scheduled. An explanation will be provided to the patient as to why he/she is being asked to have these tests, procedures, or appointments. As stated above, all interventions will be directed toward the improvement of the patients care and the avoidance of the complications of diabetes. With this document, the patient will know what his/her responsibility is to support the efforts of the team.
- For the provider, a document will have been prepared which explains the information which has been given to the nurse and the patient. The provider will be alerted to whether or not the patient has been treated to goal for diabetes and if they are not, the provider will be encouraged to change medication, life-styles, education, etc., in order to achieve control.
The Teams Activation - True Patient-Centered Care
Each team member will have access to the documents given to other members of the team. Each team member will know what is expected of the team and each team member will know the goals are for the entire team. Because the team will be spending less time on the tasks of ordering and scheduling tests, procedures and referrals, there will be more time for the building of relationships and for the engagement and activation of each member of the team.
The patient's most recent lab values are as follows.
| HbA1c | 6.5% | 05/17/2013 |
| Cholesterol | 215 mg/dL | 06/18/2013 |
| LDLC | 140 mg/dL | 06/18/2013 |
| Triglycerides | 99 mg/dL | 06/18/2013 |
| HDL | 55 mg/dL | 06/18/2013 |
The patient's lipids are not treated to goal. Take measures to move the patient toward goal of LDL < 70 mg/dL.
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
Conclusion
It takes a team to treat diabetes; without the activated, engaged participation of each team member, the entire team will fail. Below you will see the information given to your other team members. The more the entire team knows about the responsibilities of the other team members, and the more engaged each team member is with other team members, the more successfully the automated team's efforts will be.
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Patient Engagement and Activation Information
Automated Orders for Chart QTest
The following tests, procedures and referrals have been made for you. The reasons for each of them have been listed below. You will be contacted for the time and place for any referrals made.
Dilated Eye Examination
All patients with diabetes need an annual dilated examination performed by an ophthalmologist. The most common cause of blindness in the United States is uncontrolled diabetes. The annual examination allows complications to be recognized early when treatment can be undertaken to preserve your sight. Note: If a referral has been made for you and you have had a dilated eye examination in the past six months, please let your provider and/or your nurse know.
10-Gram Monofilament Examination
The most common cause of non-traumatic amputations of a limb in the United States is uncontrolled diabetes. The first step toward losing a limb is the loss of sensation in the lower extremity. It is very important that every person with diabetes has an examination of sensory perception in the lower extremity. This is done with a non-invasive examination with a 10-gram monofilament. This examination will be completed in the office by your nurse. It is an important part of the care of your diabetes.
Podiatry
All patients with diabetes should have their feet examined at each visit. In addition to the sensory examination, the feet are examined for ulcers, wounds, infections or other skin abnormalities. Patients with diabetes should not trim their own toenails, go barefoot or subject yourself to potential foot or toe injuries. If you have decreased or absence sensory perception you should be seen by a podiatrist annually. The sensory examination and proper foot care are the first steps to preserving your limbs./.
Diabetes Self Management Education (DSME) and/or Medical Nutrition Therapy (MNT)
Dr. Joslin, the founder of the Diabetes Center of Excellence, said, “The person who knows the most about diabetes will live the longest.” If you have not attended DSME classes and if you have not attended MNT classes, you must attend an initial complete course. If you have been through the complete courses, you should attend an annual refresher course. The dietician and/or Certified Diabetes Educator can help you with dietary information about diabetes, high blood pressure, cholesterol, weight reduction and many other conditions. SETMAs diabetes education program is certified by the American Diabetes Association.
Urinalysis (UA)
Because your urine is produced by the kidneys, an examination of your urine will tell your healthcare provider a great deal about the health of your kidneys. Annually, all patients with diabetes should have their urine examined for infection, protein, glucose and other abnormalities.
Micral Strip or Albumin/Creating Ratio
The most common cause of kidney failure is uncontrolled diabetes. Beyond the UA, an annual test for renal disease and/or for abnormal protein in the urine enables you and your provider to anticipate and hopefully avoid kidney problems. The micral strip and the albumin/creatinine ratio are simple non-invasive means of accessing your kidney function and the results of these tests will help you healthcare provider calculate your Estimate Glomerular Filtration Rate (eGFR) which is an even more sensitive measure of your kidney function.
Immunizations
If you have not had, or if you have refused to have an annual flu shot, an every ten-year Tdap (Tetanus, Diphtheria, Acellular Pertussus), or an every ten-year pneumonia vaccine (Pneumonvax), you should agree to these preventive measures. The increased infectious risk for patients with diabetes makes these immunizations increasingly important to maintain. Unless you are allergic to eggs, there is no medical reason for you not to have your immunizations and it is an important part of your care. Note: There is some evidence for an annual flu shot to have some cardiovascular risk benefit.
Aspirin
If you are not taking a low-dose aspirin and you are not allergic to aspirin, you should start taking an 81 mg aspiring daily. Discuss this with your healthcare provider. If you are allergic to aspirin you should not take it. If you take large doses of fish oil, Coumadin, Pradaxa or Plavix, you should discuss aspirin with your healthcare provider before taking it.
Exercise
If you are not excising routinely, you must know that nothing is more important to your health than routine exercise (walking, swimming) for 30-45 minutes four days or more a week. At SETMA you will have received a copy of your personalized exercise prescription in the LESS Initiative. Start slowly how fast you start is not as important as how consistently you exercise and work within your capacity.
Tobacco
If you smoke, or if you are exposed to tobacco smoke, your health is at significantly higher risk and you should asks your healthcare provider for help in stopping. No patient with diabetes should add to their heart disease risk by smoking.
Excess Weight
If you are overweight or obese, you should take stapes (exercise and dietary) to lose weight. Ask you provider for help. SETMAs nutritionist can give you counsel about how to change your life styles to improve your BMI and BMR (these terms are defined in your LESS Initiative.
SETMA I - 2929 Calder, Suite 100 SETMA II - 3570 College, Suite 200 Mark Wilson Clinic - 2010 Dowlen
Nederland/Port Arthur - 2400 Highway 365, Suite 201
Orange - 601 Strickland Drive, Suite 140
(409) 833-9797
www.jameslhollymd.com
Nursing Responsibilities
The following need to be completed for this patient.
10-gram Monofilament Foot Exam
Evaluation of Renal Status
Cardiometabolic Risk Syndrome Assessment
Framingham Risk Assessment
Discuss Aspirin Use
Discuss Flu Vaccination
The following tests/procedures have been automatically ordered for this patient. Be sure to send the patient to the lab and make sure they are aware of referrals that were created.
Urinalysis
Micral Strip
Request for report from previous dilated eye exam referral
Referral for DSME/MNT
| 