|
The following is a partial list of patient factors which contribute to less than optimal healthcare in the United States today:
- Lifestyle - Inactivity, poor diet, overeating, smoking, excessive alcohol consumption. Much more than genetics, lifestyle often adversely affects patient health.
- Access to healthcare - There are groups of people who have limited access to healthcare. Others cannot afford the healthcare which has been recommended. Either cause decreases or even eliminates the potential health benefit of care.
- Compliance - Patient non-compliance with prescribed treatment plans is a major problem. When patient fail to take their medications, follow-up with care as recommended or follow-through with treatment recommendations, they limit the benefit they could have received.
- Refusal - There is a difference between compliance and refusal to accept a treatment recommendation. The second most common reason for internet searches is question about healthcare. The problem is that while patients are getting more information than ever before, often that information is invalid.
- Complacency - The failure of patients to seek care or to follow known beneficial care.
Very often patients don't feel badly and as a result are unwilling to engage in uncomfortable, complicated and sometimes expensive care which can interfere with their lifestyles. The problem is that most of the illnesses which can be treated successfully but which can kill you if they aren't, don't have significant symptoms until irreversible damage has been done to your body.
In the Your Life Your Health article for April 11, 2002, entailed, "Silent Killers: Hypertension, Cholesterol Diabetes," SETMA's Managing Partner, Dr. Muhammad Aziz stated: "High blood pressure silently and slowly puts pressure on your heart, brain and kidneys, and damages them over time. You may not feel the adverse effects initially, as the process is slow. However, one day you may suddenly get chest pain and the doctor tells you that you are having a heart attack, or you have had a stroke. Then it is too late."
Boiled Frog Analogy
The boiled-frog analogy has often been used to illustrate the reluctance of people to change their behavior because they are not uncomfortable. The analogy describes a frog which is placed in a pot of cool water. The frog is comfortable and senses no danger. When the pot is placed on a stove and heat is applied, the change is so gradual that the frog is not aware of the danger until it is too late. The frog boils to death.
This is not unlike a patient who complains, "But, I was fine yesterday, why am I unable to move my left arm today?" The reason is that the patient did not take their blood pressure medication and did not control their weight and did not stop smoking until it was too late. The cause of the stroke started many years before the actual event. By the way, it is NEVER "too late" to being making changes. Recent research has shown that smokers who are diagnosed with lung cancer live longer and are more comfortable if they stop smoking than are the patients who are diagnosed with lung cancer and continue to smoke. It is NEVER too late to quit smoking.
In an attempt to get providers' to change their behavior in treating patients, SETMA;
- Tracks provider performance in the care of individual patients and makes it possible for providers to know their on every patient at the time of the patient's clinic visit.
- Audits the provider performance over the entire population of patients the provider treats.
- Analyses statistically the provider performance and compares every provider's performance with every other providers'.
- Publicly reports the providers' performance on SETMA's website.
This process increases the discomfort of providers when patients are not receiving the best care and motivates change.
Creating Discomfort in Patients
The problem remains as to how to change patient behavior. How do we make the patient uncomfortable enough that they will make and sustain changes in their lifestyles and compliance with a plan of care? One of the ways is with "risk stratification."
The calculation of a patient's risk of developing significant health problems and the showing of that calculation to the patient is one way SETMA attempts to encourage patients to make and sustain change. SETMA uses many tools to evaluate patient health risk. All are described on SETMA's website at www.jameslhollymd.com under the heading "Electronic Patient Management Tools". Two categories of risk tools are described there, under the following titles::
Preventive Heath Tools
- LESS Initiative
- Smoking Cessation
- Exercise
- Diabetic Exercise
- CHF Exercise
- Preventing Diabetes
- Preventing Hypertension
- Weight Management
Framingham Cardiovascular Risk
- Cardiometabolic Risk Assessment
- LDL Levels
- Fredrickson Classification of Dyslipidemia
- Lipid Disease Management
- Framingham Heart Study Risk Calculators
Anyone who takes the times to review these materials will learn how to improve their health and how to decrease their disease risk. One of the most valuable risk stratification tools is based on the Framingham Heart Study.
History of Framingham
In 1948, the Framingham Heart Study embarked on an ambitious project in health research to identify the common factors that contribute to cardiovascular disease by following its development over a long period of time in a large group of participants.
The Framingham Heart Disease Epidemiology Study was launched to help physicians better understand heart disease. To do this, researchers examined the lives and habits of ordinary people living in a suburban Boston town called Framingham to determine whether there was any connection between the way they lived and the health of their hearts. They investigated the risk factors that people were born with (genetic factors) and those they were exposed to (environmental factors), to see which contributed to the development of heart disease.
The researchers recruited 5,209 men and women between the ages of 30 and 62 from the town of Framingham, Massachusetts, and began the first round of extensive physical examinations and lifestyle interviews that they would later analyze for common patterns related to CVD development. Since 1948, the subjects have continued to return to the study every two years for a detailed medical history, physical examination, and laboratory tests, and in 1971, the Study enrolled a second generation - 5,124 of the original participants' adult children and their spouses - to participate in similar examinations.
In 1994, the need to establish a new study reflecting a more diverse community of Framingham was recognized, and the first Omni cohort of the Framingham Heart Study was enrolled.
In April 2002 the Study entered a new phase, the enrollment of a third generation of participants, the grandchildren of the Original Cohort. In 2003, a second group of Omni participants was enrolled.
SETMA Display of the Framingham Heart Risk Calculators
In order to utilize these tools for the benefit of our patients, SETMA has deployed all 12 of the Framingham Heart Risk Calculators in such a way that with a single click of a single button all twelve calculations are completed in less than a second.
The SETMA Framingham Heart Risk Calculators are displayed in multiple locations in our EMR including the following disease-management tool sets::
- Diabetes,
- Lipids,
- Hypertension
- CHF
- Acute Coronary Syndrome
- Chronic Stable Angina
The following is an illustration taken from the Lipids Disease Management Tool. Outlined in red is the button entitled "Framingham Risk Scores" which does the following:
- Launches the calculation of all 12 scores
- Displays them simultaneously on all of the above named disease management tools
- Places the results of the heart risk calculations on the Plan of Care and Treatment Plan which will be given to the patient
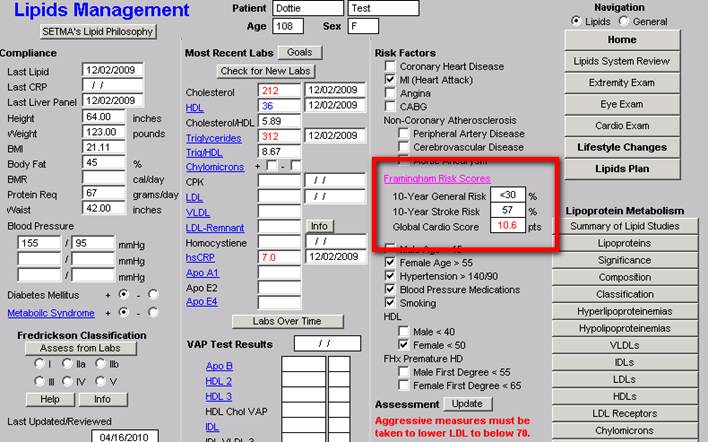
When the button entitled Framingham Risk Scores is depressed, without any other action on the provider's part, all twelve calculations are made. All data points are aggregated electronically for this purpose.
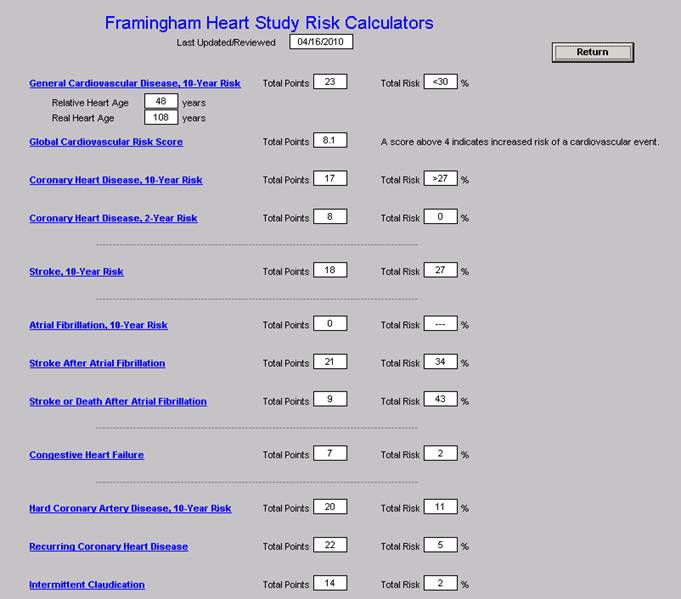
The following is the template which appears when the button entitled Framingham Risk Scores is depressed. It will be noted that the titles of each of the risk calculators is in blue. This means that each is a hyperlink and when depressed the elements on the basis of which the score is calculated is displayed. This function is a useful teaching tool, as it possible to review these elements with a patient when any score is being discussed. This will be a useful means of alerting patients to the changes they need to make in their lifestyles or treatment regimens in order to moderate their risk. The date that the Framingham Risk Scores were calculated and reviewed is noted at the top of the template.
You will note that with the General Cardiovascular Risk (10 Years) there is a calculation of the patient's "relative heart age" and a display of their age. While this calculation is not absolute, it gives SETMA's patients an indication of their heart health. The good news is that this calculation can be improved with changes in lifestyle and with appropriate and aggressive treatment.
In the following materials, an introductory statement for each of the calculations is taken from the Framingham official website at www.framinghamheartstudy.org. The Framingham statement is followed by SETMA's template which is displayed for each calculator when the hyperlinks above are launched.
The introductory material includes:
- Title of risk calculator
- Source from which it is taken
- Outcome which is the end-point for the risk calculation
- Duration of follow-up
- Population of interest
- Predictors
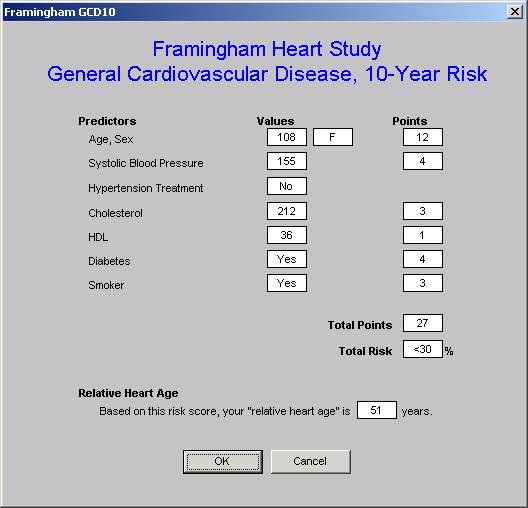
General Cardiovascular Disease (10-Year Risk)
(D'Agostino, Vasan, Pencina, Wolf, Cobain, Massaro, Kannel. 'A General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study', Circulation 2008)
Outcome -- CVD (coronary death, myocardial infarction, coronary insufficiency, angina, ischemic stroke, hemorrhagic stroke, transient ischemic attack, peripheral artery disease, heart failure)
Duration of follow-up -- Maximum of 12 years, 10-year risk prediction
Population of interest -- Individuals 30 to 74 years old and without CVD at the baseline examination
Predictors -- Age, Diabetes, Smoking, Treated and untreated Systolic Blood Pressure, Total cholesterol, HDL cholesterol, BMI replacing lipids in a simpler model.
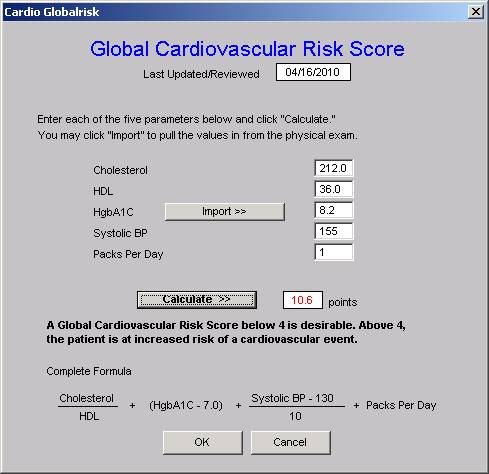
Global Cardiovascular Risk Score
This is the only risk calculator which was not published by the Framingham Heart Study. It is a modification of the risk calculator based on the Framingham data but with the elimination of age and gender. The rationale for this was that the weight of age in the Framingham study was so great that it underestimated the cardiovascular risk in the young and overestimated it in the elderly.
The Global Cardiovascular Risk Score eliminates the age and gender bias and gives a more accurate estimate of the relative risk of al groups without regard to age.
The following is the pop-up which appears when the Global Cardiovascular Risk hyperlink is launched.
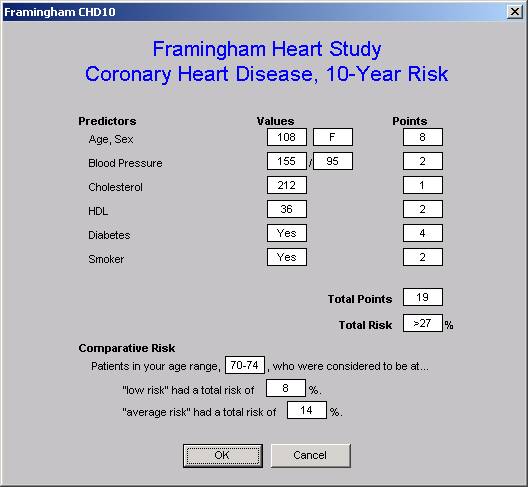
Coronary Heart Disease 10-Year Risk
(based on Wilson, D'Agostino, Levy et al. 'Prediction of Coronary Heart Disease using Risk Factor Categories', Circulation 1998)
Outcome -- Coronary Heart Disease
Duration of follow-up -- Maximum of 12 years, 10-year risk prediction
Population of interest -- Individuals 30 to 74 years old and without overt CHD at the baseline examination
Predictors - Age, Diabetes, Smoking, JNC-V blood pressure categories, NCEP total cholesterol categories, LDL cholesterol categories,
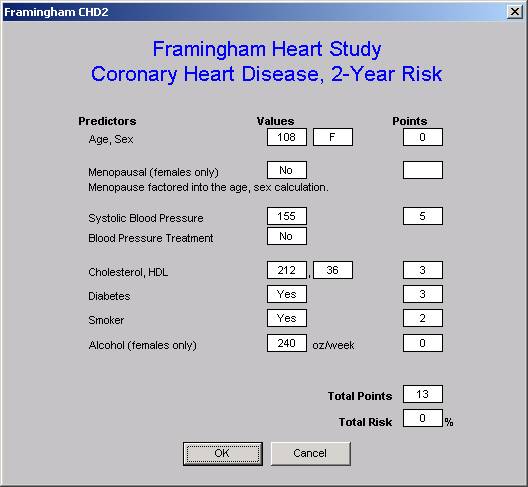
Coronary Heart Disease (2-Year Risk)
( D'Agostino, Russell MW, Huse DM et al. 'Primary and subsequent coronary risk appraisal: new results from the Framingham Study', American Heart Journal 2000)
Outcome -- First Coronary Heart Disease
Duration of follow-up -- Maximum of 4 years, 2-year risk prediction score sheets
Population of interest -- Individuals free of all of the following CVDs before examination; CHD (includes myocardial infarction, coronary insufficiency, and angina pectoris); stroke (ischemic or hemorrhagic); transient ischemic attack; congestive heart failure; intermittent claudication
Predictors - Age, Systolic blood pressure (SBP), Cigarette smoking status (1 if current smoker, 0 otherwise), Fasting lipid level (totals and HDL Cholesterol), Physician diagnosis of diabetes at the current or a previous examination, Use of antihypertensive medication (yes/no),
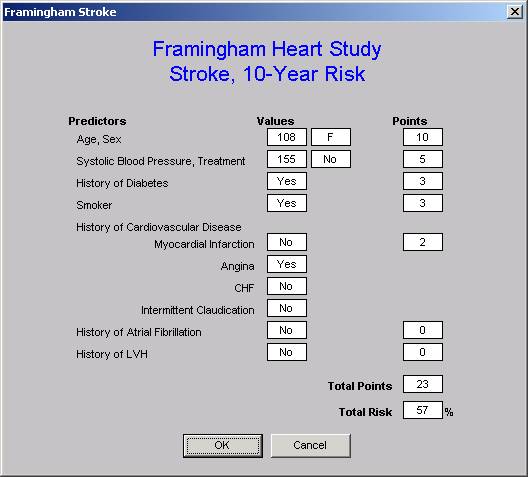
Stroke
(D'Agostino, Wolf, Belanger, Kannel 'Stroke Risk Profile: Adjustment for Antihypertensive Medication', Stroke 1994)
Outcome -- Stroke
Duration of follow-up -- 10 years
Population of interest -- Individuals aged 55 to 84 years, free of stroke at baseline
Predictors - Age, Systolic blood pressure, Diabetes mellitus, Cigarette smoking, Prior cardiovascular disease, Atrial fibrillation, Left ventricular hypertrophy, Use of hypertensive medication
All of the calculators can be reviewed on our website.
In order to improve your health, ask your healthcare provider to give you your risk scores for each of the twelve Framingham Heart Risk Calculators. Use these to guide yourself in improving your health. Remember, don't boil like a frog; jump out of the water before your health is overwhelmed.
| 