|
CMS/ONC Conference
April 23, 2015
Summary of SETMA’s Experience
by James L. Holly, MD
CMS/ONC Conference Description
- Identify desired health IT capabilities to support quality and program reporting needs for ACOs and other group reporting programs to improve health care and quality.
- Define a plan for achieving and implementing the technology and policy solutions for identified needs on a national scale.
- Provider Feedback and Engagement
- Data Capture
- Data Aggregation
- Multi-Payer Reporting
Index
Introduction
Three Overall Functionalities required to meet the goals identified by CMS/ONC
General Principles in addressing: Provider Feedback and Engagement, Data
Capture, Data Aggregation and Multi-payer Reporting
The Tracking of Quality Metrics Alone will not result in healthcare delivery transformation and/or improvement
If CMS and/or ONC Requires everyone to do everything the same way, it will potentially stifle creativity, transformation and generative thinking
Quality Metrics must be standardized in their definition and description and in data aggregation if they are going to provide data necessary for improvement of care and safety
Provider Engagement requires vision, passion and support
Specific Conceptional Ideals About the Concerns of CMS and ONC
Health IT Support for sustainable success in ACOs involve more than the fulfillment of quality metrics
Other elements of Health IT support for ACO success
Quality Metrics in health IT Support for success in ACO
The Limitations of Quality Metrics
The Number and Kind of Quality Metrics
Efforts to transform healthcare fail unless four strategies are employed.
Quality Metrics Clusters and Galaxies
The SETMA Model of Care - Brief Description
The SETMA Model Step 1 - Provider Performance Tracking - More Detail
The SETMA Model Step 2 - Auditing of Provider Performance - More Detail
The SETMA Model - Step 3 - Analysis of Provider Performance Through Statistics’ - Detail
The SETMA Model - Step 4 - Public Reporting of Provider Performance - Detail
The SETMA Model - Step 5 - Quality Assessment and Performance Improvement - detail
SETMA’s Model as a tool for Patient-Centered Medical Home
The following are my thoughts about the CMS/ONC conference April 23, 2015 in Washington, DC. This is not an attempt to document the discussions, presentations and break-out sessions, but simply for me to record my thoughts about the issues we addressed in the context of SETMA’s 20-year experience.
- Team dynamic and Being a Learning Organization - The concept of “team” and of being a “Learning Organization” from Peter Senge’s The Fifth Discipline
“Most of us at one time or another have been part of a great ‘team,’ a group of people who functioned together in an extraordinary way - who trusted one another, who complemented each other others’ strengths and compensated for each others’ limitations, who had common goals that were larger than individual goals, and who produced extraordinary results. I have met many people who have experienced this sort of profound teamwork - in sports, or in the performing arts or in business. Many say that they have spent much of their life looking for that experience again. What they experienced was a learning organization. The team that became great didn’t start off great - it learned how to produce extraordinary results.”
- Requires each of us to be better than we have ever been before
- Enables us to be better than we have ever been before
- Motivates us to be better than we have ever been before
- Allows us to take the risk of becoming better than we have ever been before
Both the surveyors and one of the executives at The Joint Commission commented about the philosophical foundation of SETMA’s work. Wednesday afternoon (March 5, 2014) I call my executive contact at The Joint Commission. He said “I was just talking to one of my colleagues and showing him SETMA’s notebook which was prepared in response to The Joint Commission’s Standards and Requirements Chapter Seven on leadership.” The executive said, “Look at this; everything they do is founded upon a philosophical foundation. They know ‘what they are doing,’ but more importantly, they know why they are doing it.’” SETMA is not the result of random efforts but of innovations and advances which are consistent with a structured set of ideals, principles and goals.
- The have a special sense of purpose that lies behind their vision and goals. For such a person, a vision is a calling rather than simply a good idea.
- They see current reality as an ally, not an enemy. They have learned how to perceive and work with forces of change rather than resist those forces.
- They are deeply inquisitive, committed to continually seeing reality more and more accurately.
- They feel connected to others and to life itself.
- Yet, they sacrifice none of their uniqueness.
- They feel as if they are part of a larger creative process, which they can influence but cannot unilaterally control. (p. 142)
- Live in a continual learning mode.
- They never ARRIVE!
- (They) are acutely aware of their ignorance, their incompetence, their growth areas.
- And they are deeply self-confident!
When the Robert Wood Johnson Foundation engaged the McColl Institute to conduct the Learning from Exemplary Practices study, 30 practices were selected from 400 nominees. SETMA was selected as one of the exemplar practices. After a four-day site visit, the survey team concluded the following:
- The fifth area of uniqueness of SETMA identified by the RWJF team was a surprise to them; it was SETMA’s IT Department. The RWJF team felt that SETMA has approached healthcare transformation differently than anyone they have seen. They related that uniqueness to the decision we made in 1999 to morph from the pursuit of “electronic patient records” to the pursuit of “electronic patient management.” They were surprised to see how centrally and essentially electronics are positioned into SETMA and how all other things are driven by the power of electronics. They marveled at the wedding of the technology of IT with clinical excellence and knowledge. The communication and integration of the healthcare team through the power of IT is novel, they concluded. The first four conclusions they reached are the following.
- The Care Coordination Department - they had never heard of such a department and had never seen one. They were impressed at how the department is integrated with the clinical personnel through electronic communication and how critical they are to our mission. Across the nation, transformative efforts in healthcare include what is referred to as “daily huddles” - meetings to discuss patient care and the days activities. They were interested in SETMA’s concept of “electronic huddles” where there is continuous communications between departments and colleagues to strengthen, coordinate and improve care.
- The Care Transition and Hospital Care Team -- The complex solutions for this critical area of practice is very impressive to them. The integration of care with the admission hospital plan of care, the discharge Hospital Care Summary and Post Hospital Plan of Care and Treatment plan, the hospital follow-up care coaching call and other aspects of this care transition process, they identified as innovative improvements in the work force relationships among staff.
- The I-Care team - they are very impressed with the electronic tools we have with which to support the work of the full time staff and the professional support staff for I-Care. SETMA has worked in the long term residential care area for its entire existence and before. But, they were impressed with how a group of SETMA providers built upon that foundation and organized an excellent integration of work flow innovations to improve that care.
- Learning Team - they believe that the spontaneous and structured learning of SETMA allows us to continually and almost unintentionally learn and grow. They understand that learning, as Senge says, is only distantly related “to taking in more information.” They believe that we have incorporated “systems thinking” and “systems structures” into SETMA extremely well. They think this is one of the most value aspects of SETMA’s work force and work flow innovations. They were able to attend one of SETMA’s monthly training meetings and were intrigued by the enthusiastic and engaged participation by all of SETMA’s healthcare providers.
- “The juxtaposition of vision (what we want) and a clear picture of current reality (where we are) generates€¦‘creative tension,’ (which is) a force to bring vision and reality together, through the natural tendency of tension to seek resolution.”
- Analytics transform knowledge into an agent for change. In reality, without analytics, we will neither know where we are, where we are going or how to sustain the effort to get there.
- For transformation to take place through knowledge, we must be prepared to ask the right questions, courageously accept the answers and to require ourselves to change.
- Healthcare transformation, which will produce continuous performance improvement, results from internalized ideals, which create vision and passion, both of which produce and sustain “creative tension” and “generative thinking.”
- Transformation is not the result of pressure and it is not frustrated by obstacles. In fact, the more difficult a problem is, the more power is created by the process of transformation in order to overcome the problem.
- The greatest frustration to transformation is the unwillingness or the inability to face current reality. Often, the first time healthcare provides see audits of their performance, they say, “That can’t be right!”
- Through analytics - tracking data, auditing performance, statistical analysis of results - we learn the truth. For that truth to impact our performance, we must believe it.
- Through acknowledging truth, privately and publicly, we empower sustainable change, making analytics a critical aspect of healthcare transformation.
- While an Electronic Health Record (EHR) has tremendous capacity to capture data, that is only part of the solution. The ultimate goal must be to improve patient care and patient health, and to decrease cost, not just to capture and store information!
- Electronic Patient Management employs the power of electronics to track, audit, analyze and display performance and outcomes, thus powering transformation.
- Public Reporting by Provider name is transformative but quality metrics are not an end in themselves.
- Optimal health at optimal cost is the goal of quality care. Quality metrics are simply “sign posts along the way.” They give directions to health.
- Metrics coupled with analytics are like a healthcare “Global Positioning System”: it tells you where you are, where you want to be, and how to get from here to there.
- Different elements of statistical analysis give different insight into population management, i.e. the mean may be at goal in a population but if the standard deviation is high, many are not to goal and efforts must be designed and made to maintain the mean while improving the SD.
- This does not impugn the setting of national standards for the capabilities of electronic medical records through a certification program.
- Neither does it oppose the setting of performance standards.
- It does suggest that CMS and ONC allow the deployment of and/or the designing of solutions required by the certification and performance standards in unique ways.
- Meaningful Use II require practices to document tobacco use by patients and the efforts of providers to confront patients about tobacco use, to counsel them about cessation of use and to document cessation methods including pharmaceuticals.
- The problem resulted from the fact that many, if not most, advance primary care practices have been doing this for years, yet the regulations required that everyone change the effective way in which they have being doing this and that they do this the same way.
- This imposed significant expense and effort in work flow changes, none of which improved outcomes.
- Another example is that the standardization of requirements without regard to unique circumstances resulted in practices like SETMA having to jerry-rig a method for meeting the penetration of use of web portals to meet imposed standards.
- This standard did not improve the quality or safety of care.
- This standard did not allow for the fact that practices such as SETMA, taking care of many people who do not have the resources to have home computer capabilities, had to manipulate their activities to meet the standard without any improvement in quality or safety but with a significant increase in cost.
- Metrics which are used must be based on good science and evidence-based treatment. They cannot be individualized and different providers cannot determine their own standards.
- Lessons which could have been learned from PQRI and PQRS
- To provide guidance for quality improvement and for safety enhancement a few metrics are not helpful. The greatest weakness of the PQRI and its successor PQRS was the impact upon quality outcomes was minimal if any because of the very few metrics required qualify for successful performance. This is discussed in great details later under SETMA’s Model of Care.
- A second deficiency of PQRS is that it missed a great opportunity to create an enormous database for improvement of healthcare in the United States. For instance, if all primary care providers had been required to report on a quality measure set on diabetes, which would have included 9-14 metrics, we would now have an enormous data based which would have allowed us to compare performance on the basis of a variety of discriminators allow the determination of best-practices.
- There must be metrics which reflect quality performance in population health as well as in the care of individuals.
- For instance, SETMA is pleased to meet the standards for Diabetes Recognition by NCQA but we are more pleased that we have been able to eliminate ethnic disparities in the care of patients with diabetes and hypertension although we have not been able eliminate disparities in Dyslipidemia.
- Currently, to my knowledge, there is no standardized reporting on ethnic disparities of care at the practice or provider level.
- The place of quality metrics and analytics in care improvement is further illustrated by the Performance Improvement Continuous Medical Education (PI-CME) program defined by the American Medical Association in 2008.
- The three steps of PI-CME are: measuring of performance, self-directed study to fill in gaps of knowledge, the re-evaluation of performance to demonstrate improvement in care based on the process.
- The PI-CME program is deficient in that it lacks a necessary fourth step for the sustaining of the performance improvement.
- That step is the development of a Clinical Decision Support which will support the sustaining of the improvement of the life of a provider’s career, also allowing for and indeed requiring modifications when new knowledge or evidence is developed.
- The automatic data capturing and data aggregation can be facilitated with intuitive disease management tools and with clinical decision support tools.
- Without knowing where you are, you can’t get to where you want to go. The thing which is lacking in healthcare today is that providers do not know how they are performing.
- If you have a GPS device which will tell you where you want to go but it will not tell you where you are, then you can’t get to your destination. You don’t know whether to go north, south, east or west or perchance you are already at your destination but you don’t and can’t know it.
- To engage providers with quality metrics and analytics they must see the necessity of both in order for them to achieve their goals.
- Once they “buy in” to the philosophy of knowing where you are in order to know how to get to where you want to go, then they will incorporate metrics and analytics into their work flow.
- Providers will resist quality metrics and analytics until their vision and their personal passion internalizes the value of these healthcare management tools.
- Providers will resist these tools unless the design and deployment of the metrics and analytics simplify their work rather than complicate it and unless they can see that metrics and analytics "make a difference" in patient health and in providers' work.
Health IT Support for sustainable success in ACOs involves much more than just the fulfillment of quality metrics. In May, 1999, SETMA defined ten principles for the development of Health IT Tools which address the issues of quality, safety, process and outcomes, i.e., which contribute to the fulfillment of the Triple Aim which was not enunciated by the Institute for Healthcare Improvement (IHI) until 9 years later. Those principles which are still relevant and valid are:
- Pursue Electronic Patient Management rather than Electronic Patient Records
- Bring to every patient encounter what is known, not what a particular provider knows
- Make it easier to do “it” right than not to do it at all
- Continually challenge providers to improve their performance
- Infuse new knowledge and decision-making tools throughout an organization instantly
- Promote continuity of care with patient education, information and plans of care
- Enlist patients as partners and collaborators in their own health improvement
- Evaluate the care of patients and populations of patients longitudinally
- Audit provider performance based on endorsed quality measurement sets
- Integrate electronic tools in an intuitive fashion giving patients the benefit of expert knowledge about specific conditions
- Health Care where the same data base is being used at ALL points of care - hospital, clinic, nursing home, home health, hospice, emergency department, providers and/or patients’ residence, etc..
- A robust EHR to accomplish the above.
- A robust business-intelligence analytics system, which allows for real-time data analysis at the point of care.
- A laser printer in every examination room so that personalized evaluational, educational and patient activation and engagement materials could be provided to every patient at every encounter, with the patient’s personal health data displayed and analyzed for individual goal setting and decision making.
- Quality metric tracking, auditing and statistical analysis.
- Public Reporting of quality metric performance by provider name.
- Quality Improvement initiatives based on tracking, auditing and analysis of metrics.
- Shared vision among all providers, support staff and administrators - a personal passion for excellence -- which creates its own internalized, sustainable energy for the work of healthcare transformation.
- Celebratory culture which does not compete with others but continually improves the organization’s own performance, using others as motivation but not as a standard.
- Monthly peer-review sessions with all providers, to review provider performance and to provide education in the use of electronic tools.
- Adequate financial support for the infrastructure of transformation.
- Respect of the personal value of all other healthcare providers regardless of level of training, and the caring for people as individuals.
- An active Department of Care Coordination and a hospital-care support team which is in the hospital twenty-four hours a day, seven days a week.
- Aggressive end-of-life counseling with all patients over fifty, and active employment of hospice in the care of patients when appropriate.
(The context of these principles and others can be found at the following link: http://jameslhollymd.com/your-life-your-health/may-1999-four-seminal-events-in-setmas-history)
- The identification of valuable quality metrics and the description and definition of them are a science. National Quality Forum, Physician Consortium for Performance Improvement (PC-PI), the National Committee for Quality Assurance (NCQA - HEDIS) and other organizations are equipped with the staff, experience and principles to identify and describe these metrics.
- Success with quality metrics will be built upon a sound philosophy and upon sound principles, some of which are:
- Quality metrics are not an end in themselves. Optimal health at optimal cost is the goal of quality care. Quality metrics are simply “sign posts along the way.” They give directions to health. And the metrics are like a healthcare “Global Positioning Service”: it tells you where you want to be; where you are, and how to get from here to there.
- The auditing of quality metrics gives providers a coordinate of where they are in the care of a patient or a population of patients.
- Statistical analytics are like coordinates along the way to the destination of optimal health at optimal cost. Ultimately, the goal will be measured by the well-being of patients, but the guide posts to that destination are given by the analysis of patient and patient-population data.
- There are different classes of quality metrics. No metric alone provides a granular portrait of the quality of care a patient receives, but all together, multiple sets of metrics can give an indication of whether the patient’s care is going in the right direction or not. Some of the categories of quality metrics are: access, outcome, patient experience, process, structure and costs of care.
- The collection of quality metrics should be incidental to the care patients are receiving and should not be the object of care. Consequently, the design of the data aggregation in the care process must be as non-intrusive as possible. Notwithstanding, the very act of collecting, aggregating and reporting data will tend to create a Hawthorne effect.
- The power of quality metrics, like the benefit of the GPS, is enhanced if the healthcare provider and the patient are able to know the coordinates while care is being received.
- Public reporting of quality metrics by provider name must not be a novelty in healthcare but must be the standard. Even with the acknowledgment of the Hawthorne effect, the improvement in healthcare outcomes achieved with public reporting is real.
- Quality metrics are not static. New research and improved models of care will require updating and modifying metrics.
- The New York Times Magazine of May 2, 2010, published an article entitled, "The Data-Driven Life," which asked the question, "Technology has made it feasible not only to measure our most basic habits but also to evaluate them. Does measuring what we eat or how much we sleep or how often we do the dishes change how we think about ourselves?"
- Further, the article asked, "What happens when technology can calculate and analyze every quotidian thing that happened to you today?" Does this remind you of Einstein's admonition, "Not everything that can be counted counts, and not everything that counts can be counted?"
- Technology must never blind us to the human. Bioethicist, Onora O'Neill, commented about our technological obsession with measuring things. In doing so, she echoes the Einstein dictum that not everything that is counted counts. She said, "In theory again the new culture of accountability and audit makes professionals and institutions more accountable for good performance. This is manifest in the rhetoric of improvement and rising standards, of efficiency gains and best practices, of respect for patients and pupils and employees. But beneath this admirable rhetoric the real focus is on performance indicators chosen for ease of measurement and control rather than because they measure accurately what the quality of performance is."
- Technology Can Deal with Disease but Cannot Produce Health
- In our quest for excellence, we must not be seduced by technology with its numbers and tables. This is particularly the case in healthcare. In the future of medicine, the tension - not a conflict but a dynamic balance - must be properly maintained between humanity and technology. Technology can contribute to the solving of many of our disease problems but ultimately cannot solve the "health problems" we face. The entire focus and energy of "health home" is to rediscover the trusting bond between patient and provider.
- In the "health home," technology becomes a tool to be used and not an end to be pursued. The outcomes of technology alone are not as satisfying as those where trust and technology are properly balanced in healthcare delivery.
- Our grandchildren's generation will experience healthcare methods and possibilities which seem like science fiction to us today. Yet, that technology risks decreasing the value of our lives, if we do not in the midst of technology retain our humanity.
- As we celebrate science, we must not fail to embrace the minister, the ethicist, the humanist, the theologian, indeed the ones who remind us that being the bionic man or women will not make us more human, but it seriously risks causing us to being dehumanized. And in doing so, we may just find the right balance between technology and trust and thereby find the solution to the cost of healthcare.
- It is in this context that SETMA whole-heartedly embraces technology and science, while retaining the sense of person in our daily responsibilities of caring for persons. Quality metrics have made us better healthcare providers. The public reporting of our performance of those metrics has made us better clinician/scientist. But what makes us better healthcare providers is our caring for people.
- The methodology of healthcare must be electronic patient management.
- The content and standards of healthcare delivery must be evidenced-based medicine.
- The structure and organization of healthcare delivery must be patient-centered medical home.
- The payment methodology of healthcare delivery must be that of capitation with additional reimbursement for proved quality performance and cost savings.
- At the core of these four principles is SETMA"s belief and practice that one or two quality metrics will have little impact upon the processes and outcomes of healthcare delivery and, they do little to reflect quality outcomes in healthcare delivery.
In the Centers for Medicare and Medicaid Services (CMS) Physician Quality Reporting System (PQRS), healthcare providers are required to report on at least three quality metrics. This is a minimalist approach to providers quality reporting and is unlikely to change healthcare outcomes or quality. PQRS allows for the reporting of additional metrics and SETMA reports on 28 PQRS measures.
- SETMA employs two definitions in our transformative approach to healthcare:
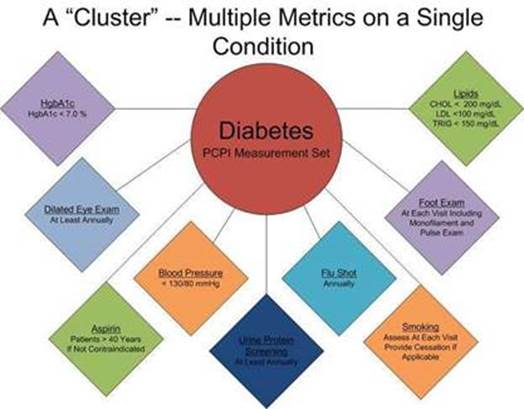
- A “cluster” is seven or more quality metrics for a single condition, i.e., diabetes, hypertension, etc.
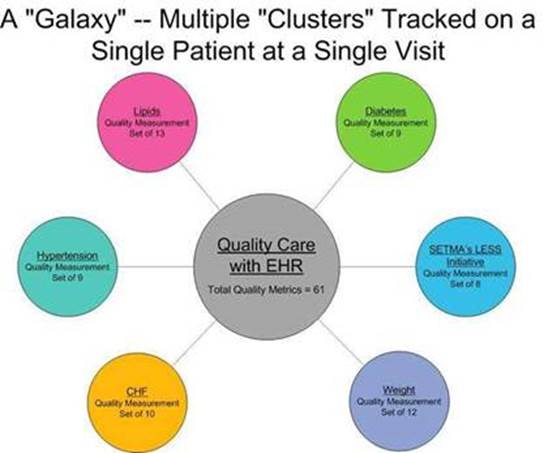
- A “galaxy” is multiple clusters for the same patient, i.e., diabetes, hypertension, lipids, CHF, etc.
- The following illustrates a “galaxy” of quality metrics. A single patient, at a single visit, may multiple “clusters” surrounding multiple chronic conditions thus having 60 or more quality metrics fulfilled in his/her care, which WILL change the quality of outcomes and will result in the improvement of the patient’s health. And, because of the improvement in care and health, the cost of that patient’s care will decrease as well.
- SETMA"s model of care is based on these four principles and the concepts of “clusters” and “galaxies” of quality metrics. Foundational to this concept is that the fulfillment of quality metrics is incidental to excellent care rather than being the intention of that care.
- The tracking by each provider on each patient of the provider’s performance on preventive care, screening care and quality standards for acute and chronic care. SETMA"s design is such that tracking occurs simultaneously with the performing of these services by the entire healthcare team, including the personal provider, nurse, clerk, management, etc.
- The auditing of performance on the same standards either of the entire practice, of each individual clinic, and of each provider on a population, or of a panel of patients. SETMA believes that this is the piece missing from most healthcare programs.
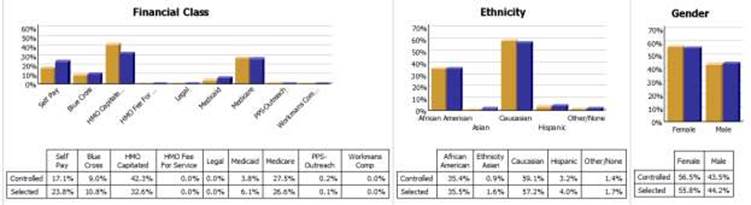
- The statistical analyzing of the above audit-performance in order to measure improvement by practice, by clinic or by provider. This includes analysis for ethnic disparities, and other discriminators such as age, gender, payer class, socio-economic groupings, education, frequency of visit, frequency of testing, etc. This allows SETMA to look for leverage points through which SETMA can improve the care we provide.
- The public reporting by provider of performance on hundreds of quality measures. This places pressure on all providers to improve, and it allows patients to know what is expected of them. The disease management tool “plans of care” and the medical-home-coordination document summarizes a patient’s state of care and encourages them to ask their provider for any preventive or screening care which has not been provided. Any such services which are not completed are clearly identified for the patient. We believe this is the best way to overcome provider and patient “treatment inertia.”
- The design of Quality Assessment and Permanence Improvement (QAPI) Initiatives - this year SETMA"s initiatives involve the elimination of all ethnic diversities of care in diabetes, hypertension and dyslipidemia. Also, we have designed a program for reducing preventable readmissions to the hospital. We have completed a Business Intelligence (BI) Report which allows us to analyze our hospital care carefully.
- The Physician Consortium for Performance Improvement (PCPI) is an organization created by the AMA, CMS, Institute of Medicine and others to develop measurement sets for quality assessment. The intent is to allow healthcare providers to evaluate their own performance at the time they are seeing a patient. SETMA is tracking a number of these measurement sets including: Chronic Stable Angina, Congestive Heart Failure, Diabetes, Hypertension, and Chronic Renal Disease Stages IV through ESRD, Adult Weight Management, and Care Transitions. Others will be added overtime. The details of these measurement sets and SETMA"s provider performance on each can be found under Public Reporting PCPI.
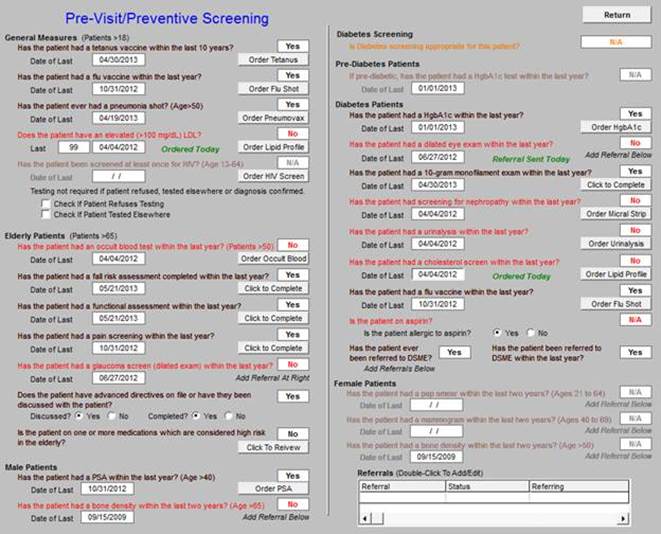
- In addition to Provider Performance Tracking tools, such as those produced by PCPI, the National Quality Foundation (see Public Reporting NQF), and National Committee for Quality Assurance (see Public Reporting HEDIS and/or NCQA), SETMA has designed a pre-visit quality measures screening and preventive care tool. This allows a SETMA provider and a patient to quickly and easily assess whether or not the patient has received all of the appropriate preventive health care and the appropriate screening health care which national standards establish as being needed by this patient.
- The following is the Pre-visit Preventive Screening tool. All measures in black apply to the current patient and are fulfilled. All measures in red apply to the current patient and have not been fulfilled and all measures in grey do not apply to the current patient. If a point of care is missing, it can be fulfilled with the single click of a single button.
- There are similar tracking tools for all of the quality metrics which SETMA providers track each day. The following is the tool for NQF measures:

- The providers" compliance with these measures is color coded for quick reference. The “view” button allows the provider to quickly review the content of the metric and to review the patient’s results.
While healthcare provider performance is important for excellent care of a patient’s health, there are 8,760 hours in a year. A patient who receives an enormous amount of care in a year is in a provider’s office or under the provider’s direct care less than 60 hours a year. This makes it clear that the patient is responsible for the overwhelming amount of their own care which includes compliance with formal healthcare initiatives and with lifestyle choices which support their health.
If responsibility for a patient’s healthcare is symbolized by a baton, the healthcare provider carries the baton for .68% of the time. That is less than 1% of the time. The patient carries the baton 99.32% of the time. The coordination of the patient’s care between healthcare providers is important but the coordination of the patient’s care between the healthcare providers and the patient is imperative.
Often, it is forgotten that the member of the healthcare delivery team who carries the “baton" for the majority of the time is the patient and/or the family member who is the principal caregiver. If the „baton" is not effectively transferred to the patient or caregiver, then the patient’s care will suffer.
Firmly in the providers hand
--The baton - the care and treatment plan
Must be confidently and securely grasped by the patient,
If change is to make a difference
8,760 hours a year.
- That the healthcare-team relationship, which exists between the patient and the healthcare provider, is key to the success of the outcome of quality healthcare.
- That the plan of care and treatment plan, the “baton,” is the engine through which the knowledge and power of the healthcare team is transmitted and sustained.
- That the means of transfer of the “baton” which has been developed by the healthcare team is a coordinated effort between the provider and the patient.
- That typically the healthcare provider knows and understands the patient’s healthcare plan of care and the treatment plan, but that without its transfer to the patient, the provider’s knowledge is useless to the patient.
- That the imperative for the plan - the “baton” - is that it be transferred from the provider to the patient, if change in the life of the patient is going to make a difference in the patient’s health.
- That this transfer requires that the patient “grasps” the “baton,” i.e., that the patient accepts, receives, understands and comprehends the plan, and that the patient is equipped and empowered to carry out the plan successfully.
- That the patient knows that of the 8,760 hours in the year, he/she will be responsible for “carrying the baton,” longer and better than any other member of the healthcare team.
- The creating of quality measures is a complex process. That is why it is important for agencies such as the Ambulatory Care Quality Alliance (AQA), the NCQA, the NQF, the Physician Quality Reporting Initiative (PQRI) and PCPI, among others, to identify, endorse and publish quality metrics. The provider’s ability to monitor their own performance and the making of those monitoring results available to the patient is important, but it only allows the provider to know how they have performed on one patient. However, the aggregation of provider performance over his/her entire panel of patients, through an auditing tool, carries the process of designing the future of healthcare delivery a further and a critical step. The problem with most auditing results, such as HEDIS, is that it is presented to the provider 12 to 18 months after the fact. SETMA believes that “real time” immediate auditing and giving of the audit results to providers can change provider behavior and can overcome “treatment inertia.”
- Auditing of provider performance allows physicians and nurse practitioners to know how they are doing in the care of all of their patients. It allows them to know how they are doing in relationship to their colleagues in their clinic or organization, and also how they are performing in relationship to similar practices and providers around the country.
- As a result, SETMA has designed auditing tools through the adaptation to healthcare of a business intelligence software. Multiple articles on SETMA"s COGNOS Project can be found under Your Life Your Health and the icon COGNOS. Those discussions will not be repeated here but auditing is an indispensable tool for the improvement of the quality of healthcare performance and for improvement in the design of healthcare delivery.
- The following are a few examples of the auditing SETMA does of provider performance.

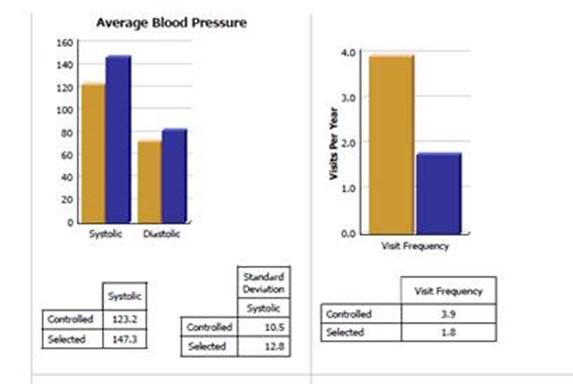
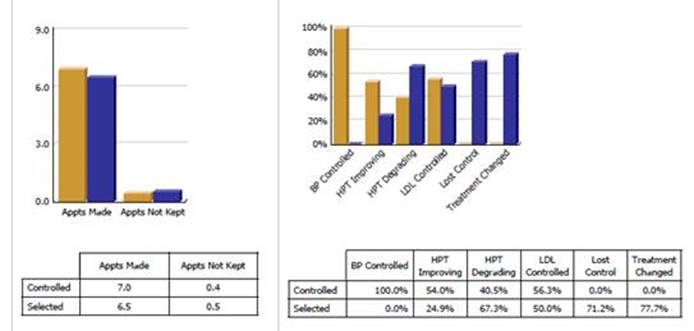
- Through BI, SETMA is able to display outcomes trending which can show seasonal patterns of care and trending comparing one provider with another. It is also possible to look at differences between the care of patients who are treated to goal and those who are not. Patients can be compared as to socio-economic characteristics, ethnicity, frequency of evaluation by visits and by laboratory analysis, numbers of medication, payer class, cultural, financial and other barriers to care, gender and other differences. This analysis can suggest ways in which to modify care in order to get all patients to goal.
- Using digital dashboard technology, SETMA analysis provider and practice performance in order to find patterns which can result in improved outcomes practice wide for an entire population of patients. We analyze patient populations by:
- Provider Panel
- Practice Panel
- Financial Class - payer
- Ethic Group
- Socio-economic groups
- We are able to analyze if there are patterns to explain why one population or one patient is not to goal and others are. WE can look at:
- Frequency of visits
- Frequency of testing
- Number of medications
- Change in treatment
- Education or not
- Many other metrics
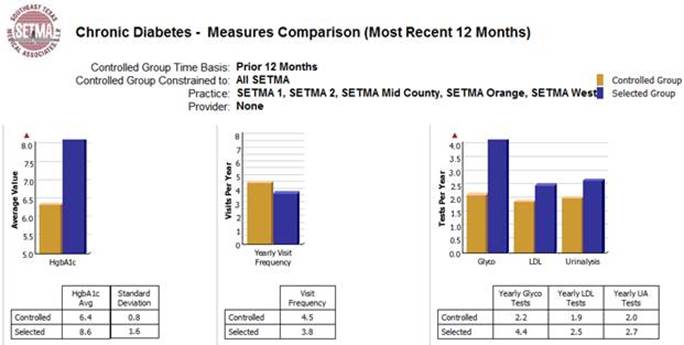
- Raw data can be misleading. It can cause you to think you are doing a good job when in fact many of your patients are not receiving optimal care. For instance the tracking of your average performance in the treatment of diabetes may obscure the fact that a large percentage of your patients are not getting the care they need. Provider Performance at the point of service is important for the individual patient. Provider Performance over an entire population of patients is important also. However, until you analyze your performance data statistically, a provider will not know how well he or she is doing or how to change to improve the care they are providing.
- Each of the statistical measurements which SETMA tracks, the mean, the median, the mode and the standard deviation, tells us something about our performance. And, each measurement helps us design quality improvement initiatives for the future. Of particular, and often, of little known importance is the standard deviation.
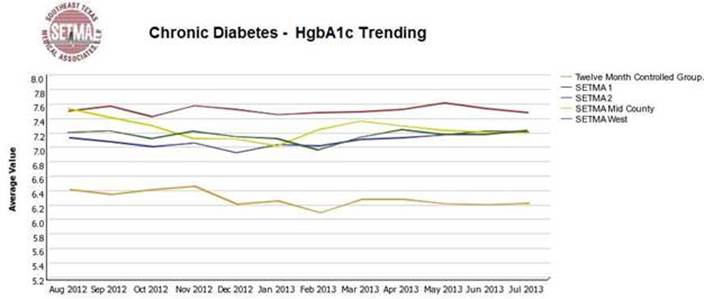
- From 2000 to 2013, SETMA has shown annual improvement in the mean (the average) and the median results for the treatment of diabetes. There has never been a year when we did not improve. Yet, our standard deviations revealed that there were still significant numbers of our patients who are not being treated successfully. Even here, however, we have improved. From 2008 to 2013, SETMA experienced a 9.3% improvement in standard deviation. Some individual SETMA providers had an improvement of over 16% in their standard deviations. Our goal for 2010 is to have another annualized improvement in mean and in median, and also to improve our standard deviation. When our standard deviations are below 1 and as they approach .5, we can be increasingly confident that all of our patients with diabetes are being treated well.
- An example of a statistical analysis of SETMA"s diabetes care in regard to the elimination of ethnic disparities of care is given in the article Eliminating Ethnic Disparities in Diabetes Care Your Life Your Life Your Health The Examiner May 13, 2010.
- One of the most insidious problems in healthcare delivery is reported in the medical literature as “treatment inertia.” This is caused by the natural inclination of human beings to resist change. Often, when patients" care is not to goal, no change in treatment is made. As a result, one of the auditing elements in SETMA"s COGNOS Project is the assessment of whether a treatment change was made when a patient was not treated to goal. Overcoming “treatment inertia” requires the creating of an increased level of discomfort in the healthcare provider and in the patient so that both are more inclined to change their performance. SETMA believes that one of the ways to do this is the pubic reporting of provider performance. That is why we are publishing provider performance by provider name under Public Reporting.
- The following is a report which appears on our website for 2009-2013 through September 30, 2013 in the NCQA Diabetes Recognition audit. All SETMA providers have earned NCQA recognition.
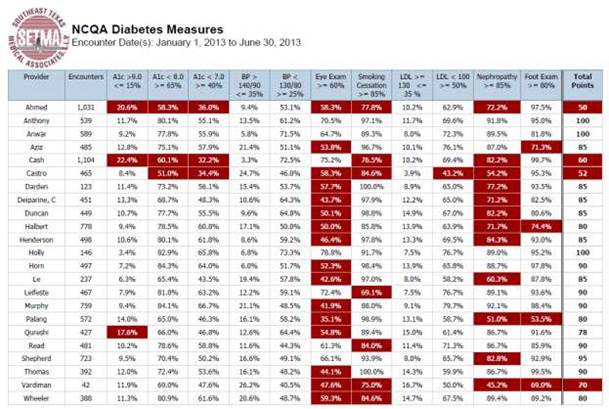
- A more complete explanation of SETMA"s philosophy and intent in “public reporting” of Provider’s performance can be found in the following articles:
Quality Improvement Initiatives based on tracking, auditing, statistical analysis and public reporting of provider performance are critical to the transformation of healthcare both as to quality of care and as to cost of care.
With the above described data in hand and with the analysis of that data, it is possible to design quality initiatives for future improvement in care. Currently SETMA is designing two major quality initiatives. One is for diabetes. It is an attempt to eliminate the last vestiges of ethnic disparity in the care of diabetes. This will require the use of additional internal resources and attention but it is our intent to do so and to permanently and totally eliminate ethnic disparities. The other is in regard to decreasing avoidable readmissions to the hospital.
The details of these two initiatives can be reviewed here:
Designing a Quality Initiative: How? Hospital Re-admissions Your Life Your Health April 29, 2010.
Eliminating Ethnic Disparities in Diabetes Care Your Life Your Life May 13, 2010
Without a systems approach to healthcare, each of these steps are impossible; certainly, the analysis and transformation of healthcare is impossible. With a systems approach, this logical and sequential process is possible and rewarding for provider and patient. This process has also set SETMA on a course for successful and excellent healthcare delivery. Our tracking, auditing, analysis, reporting and design will keep us on that course.
SETMA"s Model of Care has and is transforming our delivery of healthcare, allowing us to provide cost-effective, excellent care with high patient satisfaction. This Model of Care is evolving and will certainly change over the years as will the quality metrics which are at its core.
In February, 2009, SETMA undertook to use our Model of Care to become a medical home. In April 2010, we applied and in July, we were awarded Tier Three Medical Home recognition by NCQA and in 2013, we were again awarded the NCQA Tier III Medical Home recognition. In August, 2010 we were award Medical Home and Ambulatory Care accreditation by AAAHC and received the same for 2011-2014. This process is one of the most difficult things we have done. I use the word “is” because I believe that all of us who already have medical home “recognition” or “accreditation” or both are still in the process of transforming the practice of medicine by the principles, ideals and goals of medical home. The formal process took SETMA from February 16, 2009 to the date we first submitted our NCQA application on April 12, 2010. The process did not end there.
The transition was and is a true “transformation,” rather than a “reformation.” In function, the distinction between these two concepts as applied to healthcare is that “reformation” comes from pressure from the outside, while “transformation” comes from “an essential change of motivation and dynamic from the inside.” Anything can be reformed - reshaped, made to conform to an external dimension - if enough pressure is brought to bear. Unfortunately, reshaping under pressure can fracture the object being confined to a new space. And, it can do so in such a way as to permanently alter the structural integrity of that which is being reformed. Also, once the external pressure is eliminated, redirected or lessened, the object often returns to its previous shape as nothing has fundamentally changed in its nature.
Being from within, transformation results in change which is not simply reflected in shape, structure, dimension or appearance, but transformation results in a change which is part of the nature of the organization being transformed. The process itself creates a dynamic which is generative, i.e., it not only changes that which is being transformed but it creates within the object of transformation the energy, the will and the necessity of continued and constant change and improvement. Transformation is not dependent upon external pressure but is sustained by an internal drive which is energized by the evolving nature of the organization.
While this may initially appear to be excessively abstract and unwieldy, it really begins to address the methods or tools needed for reformation or for transformation. They are significantly different. The tools of reformation, particularly in healthcare administration are rules, regulations, and restrictions. Reformation is focused upon establishing limits and boundaries rather than realizing possibilities. There is nothing generative - creative - about reformation. In fact, reformation has a “lethal gene” within its structure. That gene is the natural order of an organization, industry or system"s ability and will to resist, circumvent and overcome the tools of reformation, requiring new tools, new rules, new regulations and new restrictions. This becomes a vicious cycle. While the nature of the system actually does change, where the goal was reformation, it is most often a dysfunctional change which does not produce the desired results and often makes things worse.
The tools of transformation may actually begin with the same ideals and goals as reformation, but now rather than attempting to impose the changes necessary to achieve those ideals and goals, a transformative process initiates behavioral changes which become self-sustaining, not because of rules, regulations and restrictions but because the images of the desired changes are internalized by the organization which then finds creative and novel ways of achieving those changes.
It is possible for an organization to meet rules, regulations and restrictions perfunctorily without ever experiencing the transformative power which was hoped for by those who fashioned the external pressure for change. In terms of healthcare administration, policy makers can begin reforms by restricting reimbursement for units of work, i.e., they can pay less for office visits or for procedures. While this would hopefully decrease the total cost of care, it would only do so per unit. As more people are added to the public guaranteed healthcare system, the increase in units of care will quickly outstrip any savings from the reduction of the cost of each unit. Historically, this has proved to be the case. When Medicare was instituted in 1965, projections were made about the increase in cost. In 1995, it was determined that the actual utilization was 1000% more than the projections. No one had anticipated the appetite for care and the consequent costs which would be created by a system which made access to care universal for those over 65 and which eliminated most financial barriers to the accessing of that care.
Reformation of healthcare promises to decrease the cost of care by improving preventive care, lifestyles and quality of care. This ignores the initial cost of preventive care which has a payoff almost a generation later. It ignores the fact that people still have the right, which they often exercise, to adopt unhealthy lifestyles. Even the President of the United States continues to smoke.
The currently proposed reformation of the healthcare system does nothing to address the fact that the structure of our healthcare system is built upon a “patient” coming to a healthcare provider who is expected to do something “for” the patient. The expectation by the system and by the recipient of care is that something is going to be done “to” or “for” the patient in which process the patient is passive. There is little personal responsibility on the part of the patient for their own healthcare, whether as to content, cost or appropriateness. The healthcare provider is responsible for the health of the patient.
Transformation of healthcare would result in a radical change in relationship between patient and provider. The patient would no longer be a passive recipient of care given by the healthcare system. The patient and provider would become an active team where the provider would cease to be a constable attempting to impose health upon an unwilling or unwitting patient. The collaboration between the patient and the provider would be based on the rational accessing of care. There would no longer be a CAT scan done every time the patient has a headache. There would be a history and physical examination and an appropriate accessing of imaging studies based on need and not desire.
This transformation will require a great deal more communication between patient and provider which would not only take place face-to-face, but by electronic or written means. There was a time when healthcare providers looked askance at patients who wrote down their symptoms. The medical literature called this "la maladie du petit papier" or “the malady of the small piece of paper.” Patients who came to the office with their symptoms written on a small piece of paper where thought to be neurotic. No longer is that the case. Providers can read faster than a patient can talk and a well thought out description of symptoms and history is an extremely valuable starting point for accurately recording a patient’s history. Many practices with electronic patient records are making it possible for a patient to record their chief complaint, history of present illness and review of systems, before they arrive for an office visit. This increases both the efficiency and the excellence of the medical record and is part of a transformation process in healthcare delivery.
This transformation will require patients becoming much more knowledgeable about their condition than ever before. It will be the fulfillment of Dr. Joslin’s dictum, “The person with diabetes who knows the most will live the longest.” It will require educational tools being made available to the patient in order for them to do self-study. Patients are already undertaking this responsibility as the most common use of the internet is the looking up of health information. It will require a transformative change by providers who will welcome input by the patient to their care rather seeing such input as obstructive.
This transformation will require the patient and the provider to rethink their common prejudice that technology - tests, procedures, and studies - are superior methods of maintaining health and avoiding illness than communication, vigilance and “watchful waiting.” Both provider and patient must be committed to evidence-based medicine which has a proven scientific basis for medical-decision making. This transformation will require a community of patients and providers who are committed to science. This will eliminate “provider shopping” by patients who did not get what they want from one provider so they go to another.
This transformation will require the reestablishment of the trust which once existed between provider and patient to be regained. That cannot be done by fiat. It can only be done by the transformation of healthcare into systems which we had fifty to seventy-five years ago. The patient must be absolutely confident that they are the center of care but also they must know that they are principally responsible for their own health. The provider must be an extension of the family. This is the ultimate genius behind the concept of Medical Home and it cannot be achieved by regulations, restrictions and rules.
The transformation will require patient and provider losing their fear of death and surrendering their unspoken idea that death is the ultimate failure of healthcare. Death is a part of life and, in that, it cannot forever be postponed, it must not be seen as the ultimate negative outcome of healthcare delivery. While the foundation of healthcare is that we will do no harm, recognizing the limitations of our abilities and the inevitability of death can lead us to more rational end-of- life healthcare choices.
|
