|
Table of Contents
November 20, 2015
Amy Townsend, MD
Vice President Medical Affairs
Christus St. Elizabeth
Dear Dr. Townsend
The following is your charge to Dr. Anwar and to me. You stated that, ““I feel it is imperative for SETMA to give specific examples of how the RN taking call is able increase efficiency but yet remain compliant with the rules in the Nurse Practice Act.” This is my response.
In the midst of a months-long effort on the part of the Medical Executive Committees (MEC) of two Southeast Texas hospitals to limit the activities of registered nurses (RN), this is Dr. Townsend’s question to SETMA; I shall attempt to answer it. The foundation of my answer began with SETMA’s beginning and a significant aspect of the MECs’ actions can be found in the history of physicians responses to nurses.
Before SETMA understood that Twenty-First Century medicine could not be practiced with “pencil and paper” (19th Century Medical Record Methodology), or even with “dictation and transcription” (20th Century Medical Record Methodology), both of which drove SETMA to Electronic Medical Records in 1998, SETMA understood that the demands of 21st Century medicine would require a team approach to healthcare delivery. The principles of “team care” have been repeated and refined but they have been part of the organizational spirit of SETMA from the beginning. That team led us to a significant examination of the value of each member of the team and to their contribution to SETMA’s model of care. Without this team concept and reality, SETMA would not be where it is today.
As the discussion of RNs’ roles in inpatient care has grown, it has become apparent that the approach of some MEC members has followed their personal established patterns of practice with no further standard or validation. Dr. Townsend voices support for the positions of some members of the MEC on the qualification that they are active in the Texas Medical Association (TMA). One person is an anesthesiologist. The reality is that while the TMA is a noble organization, like the American Medical Association (AMA), it largely exists to protect the prerogatives of physicians. And, while anesthesiologists contribute significantly to the excellence of care in SE Texas, no group has been more active at the national level in opposing the expansion of the role of nurses than anesthesiologists.
Their activities in regard to Nurse Anesthetists predispose them to argue against any expansion of the roles of nurses in healthcare. While speaking at the AMA several years ago, I sat in on a plenary session of the House of Delegates. One of the points of discussion was the role of Nurse Anesthetist. The discussion revolved around limiting their role and concluded with a former Nurse Anesthetist, having become an Anesthesiologist, declaring “if they want to practice medicine, let them go to medical school.” At that moment, I realized this debate was not about protecting the safety of the public; it was about protecting the turf of the anesthesiologists.
In 2010, the Coordinating Board for Texas Higher Education held hearings concerning expanding nursing education at two Texas Health Science Centers to include the Doctor of Nurse Practitioner degree. A Texas specialist (not an anesthesiologist) testified before the Coordinating Board opposing the expansion. In his testimony he summarized his position by saying, “Nurses should go back to bed pans and giving enemas.” This reactionary position seemed very similar to the above AMA discussion which was focused more on the turf of doctors than the protection of the public health. SETMA supported the degree programs implementation - which was passed - our input can be reviewed at:
http://jameslhollymd.com/Letters/Coordinating-Board-Texas-Highter-Education-DNP-Letter-in-support-of-the-DNP-program.
Historically, in Southeast Texas, it was cardiologists who over 30 years ago employed RNs in the hospital to facilitate continuity of and transition of care, particularly in regard to medication reconciliation. That is why it is difficult to understand the reason for their now wanting to turn the clock back to solo, isolated physicians operating alone in a complex healthcare environment which requires team for excellent functioning.
In order to create great teams, the educational process has to change: see http://jameslhollymd.com/Your-Life-Your-Health/Medical-Home-Part-V-Healthcare-education-and-healthcare-Delivery-Changes-needed-in-both. The ideal setting in which to deliver and to receive healthcare is one in which all healthcare providers value the participation by all other members of the healthcare-delivery team. In fact, that is the imperative of Medical Home. Without an active team with team consciousness and team collegiality, Medical Home is just a name which is imposed upon the current means of caring for the needs of others. And, as we have seen in the past, the lack of a team approach at every level and in every department of medicine creates inefficiency, increased cost, potential for errors and it actually eviscerates the potential strength of the healthcare system.
Why is this? Typically, it is because healthcare providers in one discipline are trained in isolation from healthcare providers of a different discipline. Oh, they are in the same buildings and often are seeing the same patients but they rarely interact. Even their medical record documentation is often done in compartmentalized paper records, which are rarely reviewed by anyone but members of their own discipline. This is where the first benefit of technology can help resolve some of this dysfunction. Electronic health records (EHR), or electronic medical records (EMR) help because everyone uses a common data base which is being built by every other member of the team regardless of discipline. While the use of EMR is not universal in academic medical centers, the growth of its use will enable the design and function of records to be more interactive between the various schools of the academic center.
And, why is that important? Principally, because more and more healthcare professionals are discovering that while their training often isolates them from other healthcare professionals, the science of their disciplines is crying for integration and communication. For instance, there was a time when physicians rarely gave much attention to the dental care of their patients, unless they had the most egregious deterioration of teeth. Today, however, in a growing number of clinical situations, such as the care of diabetes, physicians are inquiring as to whether the patient is receiving routine dental care as evidence-based medicine is indicating that the control of disease and the well-being of patients with diabetes are improved by routine dental care. Also, as the science of medicine is proving that more and more heart disease may have an infectious component, or even causation, the avoidance of gingivitis and periodontal disease have become of concern to physicians as well as dentist.
In addition, Medical Home places major emphasis upon issues which historically have been the concern of nurses. Physicians who use EMRs are discovering that the contribution of nursing staff can make the difference in the excellent and efficient use of this documentation and healthcare-delivery method. No longer is the nurse a "medical-office assistant" ancillary to the care of patients, but the nurse is a healthcare colleague central and essential to the patient's healthcare experience. As evidence-based medicine expands the scope of what The Innovator's Prescription: A Disruptive Solution for Health Care By Clayton M. Christensen labels as "empirical medicine" which ultimately leads to "precise medicine," it is possible for physicians and nurses to be a true-healthcare delivery team, as opposed to the nurses only being an aide to the physician.
Christensen identifies the following "Levels of medicine" and makes the following judgments about the future of healthcare delivery:
- Intuitive Medicine -- "When precise diagnoses isn't possible...where highly trained and expensive professionals solve medical problems through intuitive experimentation and pattern recognition."
- Empirical Medicine -- "As patterns become clearer, care evolves into the realm of evidence-based medicine...where data are amassed to show that certain ways of treating patients are, on average, better than others."
- Precise medicine -- "When diseases are diagnosed precisely...therapy that is predictably effective ... (can) be developed and standardized."
Change wrought by Precision Medicine
- “... (When) we know what type of bacterium, virus, or parasite causes one of these disease..."
- “... (When) we know the mechanism by which the infection propagates..."
- "...Predictably effective therapies can be developed..."
- "...Therapies that address the cause, not just the symptoms..."
As a result, Christensen concludes:
- "...nurses can now provide care for many infectious diseases..."
- "...patients with these diseases only rarely require hospitalizations."
It is easily recognized in this emerging paradigm that all of the schools in the academic healthcare center are actively involved in patient care and in the training of those who will be healthcare providers. Yet, it seems that the farther and farther a person advances in biomedical education, the obvious union of their disciplines at their foundations seems to be lost and the more isolated from the whole these "specialists" and “experts" become. This even creates problems within the various disciplines as egocentrism isolates one medical specialty from another. It is as a result of the need for the integration of healthcare disciplines at the delivery level, that the imperative becomes obvious for the restructuring of the training of the members of this healthcare team. And, the first change must come in the relationships between the leaders of the training programs who educate and mentor future healthcare scientist, teachers, caregivers and researchers. The educational leaders must model this integration for their disparate student bodies and that modeling will require the investment of the most precious and rare resource: time.
This is not the law of the land but it will be in the future.
What is the model for this restructuring of the relationships between schools in the academic healthcare centers? It has been suggested that there is "glue" which unites the members of the various schools which will ultimately create this team. I would argue with that. Glue is an adherent. In this context, "adherence" is described and simultaneously defined by the following: "Two dissimilar parts touching each other but not fused." "The union of separate parts; tending to adhere to or be connected by contact." If propinquity -- the state of being close to someone-- is the principle motivation for the forming of a team, it will not survive the stresses and pressures which tend to make the team fly apart.
On the other hand, "cohesion" is "the bonding together of members of an organization/unit in such a way as to sustain their will and commitment to each other, their unit, and the mission," and it has been further defined as a "union between similar plant parts or organs." Synonyms of "cohesion" are "harmony, agreement, rationality." Here is the source of the union of the various elements of the healthcare team in training. It is in the recognition of their commonness and in the acknowledgment of their being part of the same "organism."
The concept of "harmony" is valuable here also. Harmony is not the absence of discord; it is the presence of a common nature. The typical definition for a harmonic is "a sinusoidal component of a periodic wave or quantity having a frequency that is an integral multiple of the fundamental frequency." I smiled and chuckled aloud as I wrote this last sentence. It is a mouthful, but how is it related to our problem of healthcare delivery? If you have a room filled with tuning forks of different frequency and you strike one of the forks, all of the forks which are of the same frequency or a multiple of the same frequency, as the one struck, will begin to sound. Those which are intrinsically different will remain silent.
In a room of educators, some health science, some historians, some vocalists, some archeologists, etc., when the sounding is of excellence in healthcare delivery; when the sounding is of evidence-based medicine; when the sounding is of containing the cost of healthcare while maintaining the quality; when the sounding is of increasing the accessibility of healthcare by removing barriers of affordability, linguistics, literacy, etc; each member of the healthcare-education team, whether nurse, dentist, physician, scientist, physical therapist, laboratory technician or other, will begin to resonate, as they are all coherent, by their nature, to the process of sustained improvement in the delivery of healthcare. It is as if the healthcare-education team, as the healthcare-delivery team, has become a symphonic orchestra made up of instruments which are different in sounding method but which harmonize to produce an aesthetically satisfying result. Remember, the Greek word "symphonia" means "sounding together." So it is that the members of the healthcare-education and the healthcare-delivery team "resonate together" to produce the results we all desire.
My personal pilgrimage in this process began my first year in medical school, but it was not in the class room. One day, as I was leaving the medical school with a classmate, the Dean's secretary ran up to us and said, "Larry, you must go downstairs. There is a meeting for the new health careers program and the Dean is there by himself." Reluctantly, I went and began a two-year participation in the School of Medicine's Health Careers Program and a life-time of desire to help young people pursue health careers. Every Saturday, we brought high school students, principally Hispanics, to the school of medicine and introduced them to health careers. I realized then that the recruitment of a diverse student body to the various elements of the health science center was not going to be done en masse but it was going to be done one student at a time. As a result, one of the missions of the SETMA Foundation is to help underwrite the education costs for students who qualify but cannot afford health-career education.
The second element to my pilgrimage was in Clifton, Texas, after graduation from Medical School. With the birth of my second child days before graduation and with him in neonatal ICU, I had to work in order to provide for my family. Monday after gradating on Saturday, I left for Clifton. I lived in the hospital around the clock with two days off in a month to take the state medical boards. I learned the value of a healthcare team from an LVN when one night, as I was preparing to treat a patient in the ER, she said, "I have noticed that our doctors do that this way." She was so kind. She didn't say, "Hey, stupid, didn't you learn anything in medical school?" Yet, over the next four weeks, my wealth of knowledge of physiology, pathophysiology, biochemistry, heart failure, etc., was augmented by a wealth of practical medicine taught to me by an LVN. What doctor cannot remember the same kind of experience with a nurse, or other healthcare team member who helped him/her through a patient encounter which was new? Why have we forgotten?
The third element of my pilgrimage was SETMA's migration to EMR. When SETMA was formed there was no uniformity in how medical records were created, filed or stored. Some dictated records, others hand wrote records. Some organized records alphabetically, others used a numeric system. On August 1, 1995, SETMA's medical-record-keeping illustrated all of the problems facing the future of healthcare in America. With the new millennium approaching, with all of the potential of 21st-Century technological care, SETMA was hamstrung by the use of mixture of a 19th -Century documentation system, i.e., pencil and paper, and a 20th-Century system, i.e., dictation and transcription. Neither system was capable of supporting innovation in healthcare delivery. In March of 1998, we purchased an EMR system.
Two events define our success with NextGen EMR and EPM. They occurred simultaneously. The first was our realization that this task was too hard and too expensive if all we were to get out of it was the ability to document a patient encounter electronically. It was this realization which pushed us past electronic patient records to electronic patient management. We realized that we had to develop the functionality for the EMR to enhance the quality of patient care, to increase the satisfaction of patients themselves and to expand the knowledge and skills of health care providers, if it was to be "worth it." It also had to expand the healthcare team to include all participants as active, valuable contributions to the delivery of healthcare. In the spring of 1999, we made this transition to electronic patient management and the investment of time and money suddenly was "worth it."
The second event occurred in May, 1999, and it set the tone for the next ten years of EMR implementation. In a moment of frustration at the new system, which at this point of development was cumbersome to use and yielded little more than an acceptable record of a patient encounter, one partner said, "We haven't even begun to crawl yet," speaking of our use of the EMR. SETMA's CEO said, "You're right, but let me ask you a question. When your oldest son first turned over in bed, did you lament to your wife, 'this retarded, spastic child can't even walk, all he can do is turn over in bed,' or did you excitedly announce to your wife, 'he turned over in bed!'?" He smiled and the CEO added, "If in one year, all we're doing is what we are presently doing, then I'll join you in your complaint. For now, I am going to celebrate the fact that we have started and that we are doing more than before."
That celebratory attitude has given SETMA the energy and resolve to face hard times and the vision of electronic patient management has given us direction and substance to our goal. Today, we are not what we were, and we are not yet what we shall be, but we are on a pilgrimage to excellence which will never end. We started eight years ago at MGMA; where is the end? There isn't one and that is what helps us get up day after day, excited about the prospect of the future. Mostly what we celebrate today is the team which EMR has facilitated our forming.
Now, we come to Medical Home. As the healthcare education establishment is reorganizing itself to model the health-care-team concept for those they are teaching and mentoring, those in healthcare delivery are enjoying the opportunity to rethink our approach. Many of us have already experienced through the implementation the value of a healthcare team. Now with the power of the EMR, we have embedded HEDIS standards and other measures of quality into our EMR. We have designed a Coordination of Care review which allows us a snapshot at every visit as to where our patients are in their healthcare journey. We have completed a 408-page review of our practice and have been able to analyze what we are doing well and where we need to improve. Most of all, we have recognized how valuable the healthcare team is to our model of healthcare delivery and how central it is to Medical Home.
We value participants in healthcare delivery by what we pay them, but more essentially we value them by how we treat and relate to them. In the future, healthcare will undergo significant changes in monetary valuation of services which have been delivered. That will be forced upon us. However, our valuation of the contribution of others to our team is within our power to judge and acknowledge. How well and accurately we do that, to a great extent, will determine how we navigate the future.
In 2009, SETMA began studying the PC-MH model of practice organization and dynamic. The motivation for this was the challenge to create a healthcare team with the patient and all healthcare professionals as members of that team. Athletic metaphors are commonly used in analyzing life situations. Often they are overstated and/or overused, but there is one place where an athletic metaphor is apt in defining a critical point in healthcare. That is in the 'transitions of care' from one venue of care to another. The metaphor is found in track and field relay races.
No matter how talented the members of a relay team are, the most critical point of their collective performance is in the transition of the race from one runner to another. At this point, one runner, moving as fast as he/she can, must hand the baton to another runner, who has started running as fast as he/she can, before the first runner has even arrived in the "transfer zone." As if this were not complex enough, the rules of the race require that the transfer of the baton must take place within a certain zone.
If the baton is dropped or if the transfer is not made in the prescribed time, the team, no matter how gifted, will be disqualified and will lose the race. As with life and with healthcare, it is not always the brightest, fastest, or best person who wins. It is the person, in this case, the team, which not only performs well in their individual area of responsibility but who also performs well in transferring the results of his/her performance to the next participant and who does so within the constraints of the rules. Often, it is forgotten that the member of the healthcare delivery team who carries the 'baton' for the majority of the time is the patient and/or the family member who is the principal caregiver. If the 'baton' is not effectively transferred to the patient or caregiver, then the patient's care will suffer."
In 2010, SETMA sought and received “recognition” by the National Committee for Quality Assurance (NCQA) for PC-MH as the highest level. Subsequently, SETMA has received accreditation for ambulatory care and PC-MH by the Accreditation Association of Ambulatory Healthcare (AAAHC), URAC and the Joint Commission. To date, SETMA is the only practice in America which is accredited by all four. We have renewed all accreditations at three year intervals and will do so again in 2016 and 2017. (These accreditations can be reviewed at http://jameslhollymd.com/accreditations)
SETMA’s commitment to a “team approach” to healthcare is the core principle of our existence and is one of the reasons we so aggressively resist attempts to dismantle or to emasculate our team.
In April, 2012, the Robert Wood Johnson Foundation (RWJF) requested information from SETMA in anticipation of RWJF selecting 30 practices in America for a program entitled The Primary Care Team: Learning from Exemplar Ambulatory Practices (LEAP) (see: http://jameslhollymd.com/In-The-News/pdfs/primary-care-rjwf-april-2012.pdf). SETMA submitted a sixty-page summary of SETMA’s work (see: http://jameslhollymd.com/Letters/robert-wood-johnson-foundation-pct-leap). Subsequently, SETMA was selected as one of the thirty (see: http://jameslhollymd.com/in-the-news/Project-LEAP-Award). On May 30, 2012, SETMA presented a five-part series on this work beginning with the following link, with the other four shown at the bottom of the first: http://jameslhollymd.com/Your-Life-Your-Health/SETMA-Response-RWJF-Part-I-The-Primary-Care-Team-Learning-From-Effective-Ambulatory-Practices.
The Following Note is from 2012
On November 1, 2012, The Robert Wood Johnson Foundation site visit team exited SETMA about 4:30 PM. They had nothing but positive things to say about SETMA and they feel that they learned a great deal which will advance their project. They plan to have a formal report to us by the first of January. When that comes a number of you will be asked to review it and to comment on it.
The over arching analysis is they were impressed that everyone they talked to said that they are constantly trying to improve what we are doing. They were complimentary of all of our staff addressing how insightful and bright they are and also how friendly. They particularly address our front office people whom they felt really like people and try to make everyone welcome.
They identified five areas which were most impressive to them, each of which involves a different perspective of SETMA’s team:
- The Care Coordination Department - they had never heard of one and never seen one. They were impressed at how the department is integrated with the clinical personnel through electronic communication and how critical they are now to our mission.
- The Care Transition and Hospital Care Team -- The complex solutions for this critical area of practice is very impressive to them. (Of note, this is the focus of the pressure against SETMA’s team work which is coming from the hospital’s MEC.)
- The I-Care team - they are very impressed with the electronic tools we have with which to support the work of the full time staff and the professional support staff for I-Care (Nursing Home).
- Learning Team - they believe that the spontaneous and structured learning of SETMA allows us to continually and almost unintentionally learn and grow. They understand that learning, as Senge says, is only distantly related to taking in more information. They believe that we have incorporated systems thinking into SETMA extremely well. They think this is one of the most valuable things about SETMA.
The fifth area was a surprise to them and that is our IT Department. They said that we have approached healthcare transformation differently than anyone they have seen. They related that to the decisions we made in 1999 to morph from the pursuit of electronic patient records to the pursuit of electronic patient management. They were surprised to see how centrally and essentially electronics are positioned into SETMA and how all other things are driven by the power of electronics. They marveled at the wedding of the technology of IT with clinical excellence and knowledge. One of the “work force changes which are recommended for Medical Home are ‘daily huddles” where providers get together to discuss patients. I suggest and I believe that SETMA has a virtual and a virtually continuous electronic huddle all day long.
I am very impressed with how much the team learned about SETMA in such a short time. In the exit interview and at many other times in our conversations, we addressed Peter Senge’s concept of personal mastery. Senge declares: "All too often, teams in business tend to spend their time fighting for turf, avoiding anything that will make them look bad personally, and pretending that everyone is behind the team’s collective strategy - maintaining the appearance of a cohesive team."
The deception employed here is the illusion of competence. It is never popular to say, “I don’t know,” but sometimes it is the most creative approach to solving a problem. The admission that you don’t know, or that the “management team” does not know, often makes the team aware of possibilities which otherwise would be excluded. This is the foundation of the last three characteristics of “personal mastery” which Senge addresses in The Fifth Discipline. People who have a high degree of personal mastery have the following ten characteristics:
- They have a special sense of purpose that lies behind their vision and goals. For such a person, a vision is a calling rather than simply a good idea.
- They see current reality as an ally, not an enemy. They have learned how to perceive and work with forces of change rather than resist those forces.
- They are deeply inquisitive, committed to continually seeing reality more and more accurately.
- They feel connected to others and to life itself.
- Yet, they sacrifice none of their uniqueness.
- They feel as if they are part of a larger creative process, which they can influence but cannot unilaterally control.
- They live in a continual learning mode.
- They never ARRIVE!
- (They) are acutely aware of their ignorance, their incompetence, and their growth areas.
- And they are deeply self-confident!
I think these elements of personal mastery describe the culture of SETMA and explain a great deal of our success. But, how can you be “deeply self-confident” and yet be “acutely aware of your ignorance and incompetence?” It is that very contradiction which is the foundation of a learning organization. If we are going to move forward in medical informatics, we will have to be part of such a team. We will move confidently, but in that we have a degree of incompetence, we move forward to create a future of our own design. If the health care industry is going to design its own future by solving "the" problems, it means that we must develop a collaborative, learning team.
Both the surveyors and one of the executives at The Joint Commission commented about the philosophical foundation of SETMA’s work. Wednesday afternoon (March 5, 2014) I called my executive contact at The Joint Commission. He said “I was just talking to one of my colleagues and showing him SETMA’s notebook which was prepared in response to The Joint Commission’s Standards and Requirements Chapter Seven o leadership.” The executive said, “Look at this; everything they do is founded upon a philosophical foundation. They know ‘what they are doing,’ but more importantly, they know why they are doing it.’” SETMA is not the result of random efforts but of innovations and advances which are consistent with a structured set of ideals, principles and goals.
In October, 2012, SETMA’s CEO addressed a primary care conference entitled, “Empowering Future Physicians Conference: American Student Medical Association University of Texas Health Science Center San Antonio School of Medicine.” The theme of his presentation was, “The Dimensions and Dynamic of Primary Care In The Future: Harnessing the Unique Skills of a Multi-Disciplinary and Interdepartmental Team in the Transformation of Healthcare.” Some of the concepts presented in that presentation were:
- Primary care providers will define new “models of care” and with experimentation and innovation will improve the healthcare system.
- This is illustrated by a primary-care-dominated, multi-specialty care group in Southeast Texas.
- Created on a collaborative, team model, SETMA’s primary care team includes nurse practitioners, nurses, specialized (but not specialty) care delivery teams, administrative staff and physicians.
- Primary care physicians have been part of the major changes which have taken place in medicine. Now primary care physicians are resisting the changes being caused by nurse practitioners and by physician assistants.
- There are some things which NPs and PAs do better than physicians.
- First Step: Can we all agree to stop using the condescending and patronizing terms “physician extenders” and “mid-level providers?”
The full address can be reviewed at: http://jameslhollymd.com/Presentations/Primary-Care-The-Future-of-Medicine.
The health care team is larger today than ever before and it is only growing. Dr. Holly also delivered the 2013 Commencement Address to the University of Texas Health Science Center at San Antonio School of Health Professions (see http://jameslhollymd.com/Presentations/Commence-Address-School-of-Health-Professions). Eight healthcare disciplines are part of the School of Health Professions. They are:
- Clinical Laboratory Sciences
- Cytogenetics
- Dietetics
- Emergency Health Sciences
- Occupational Therapy
- Physical Therapy
- Physician Assistant Studies
- Respiratory Care
One health science center executive responded to the address with the following comment: “You did such a wonderful job speaking to each SHP program and the value they add to the healthcare team. I nearly burst with pride!” The technical competence of each of these disciplines are such that it is not uncommon to see physicians writing referrals with the following instructions: “evaluate and treat.” Increasingly, the technical expertise of each discipline will be recognized and their judgment will be sought. This is the way a team ought to work.
Also, in 2012, Dr. and Mrs. Holly in association with SETMA endowed the first PC-MH Distinguished Chair at the University of Texas Health Science Center at San Antonio. The Chair is an inter-departmental and inter-disciplinary endowment to promote primary care, PC-MH and collaboration between the School of Medicine and the School of Nursing. Additional endowments by Dr. and Mrs. Holly were for a Distinguished Visiting Professorship which supports an annual teaching and dialogue by a visiting professor on the same subjects. Another endowment was created for The Primary Care Institute at San Antonio.
In January, 2013, SETMA published a description of our hospital care team as the hospital in dealing with unacceptable practices by some, sought to dismantle SETMA team. (see http://jameslhollymd.com/your-life-your-health/inpatient-team-based-care-process-analysis).
That article said in part the following: (Author’s Note: Following a CMS hospital survey several questions were raised about how physicians and nurses share their work. The survey team was alarmed that some physicians were allowing Registered Nurses with Associate Degrees (2 year diplomas) to complete patient evaluations. While SETMA’s work was lauded, because SETMA is committed to changing how various members of the healthcare team relate to one another, this allowed SETMA to re-think our team-approach to inpatient-healthcare delivery. This is an analysis of the process SETMA employs in the hospital.)
SETMA’s team approach to inpatient care is a success as demonstrated by the facts that our lengths of stay, quality metrics, cost of care and patient satisfaction are excellent. And, it is one of the reasons why the indigent, uninsured and unassigned patients for whom we care receive the same quality of care as our private patients. I would offer the following observations about SETMA’s team. SETMA has licensed and credentialed healthcare professionals who work to the top of, but not beyond their legal scope of practice as defined by each of their accreditation agencies.. As a policy issue, the prestigious and influential Health Affairs publication of January 14, 2013, published an extensive article entitled, Primary Care Physician Shortages Could Be Eliminated Through Use Of Teams, Non-physicians, And Electronic Communication” The goal of this transformation is to integrate the teams to increase their efficiency, excellence and economy. This is what SETMA started eighteen years ago.
Fundamental to this entire discussion is the “change of mind” which healthcare providers and surveyors must have. This metanoia (change of mind) must take place in order for surveyors to distinguish between the excellence of the new and the excesses and abuses of the past, which may at first glance seem similar. They must know that SETMA’s patients are not treated in isolation, as patients have traditionally been treated. Traditionally, medical records were locked up in the providers’ offices, or in the hospital’s medical records department. To judge SETMA by the state of care given by healthcare providers who do not have an integrated delivery system with robust electronic patient management is to do a disservice to all of us.
In the emergency department (ED) and in the hospital, traditionally, the only data continuity was provided by the availability of old hospital admission records. The problem with those records is that there may be several years of time and dozens of visits and modifications of the patient’s treatment plan, since the last hospitalization. So, at best the available records were incomplete and at worst were so outdated they were useless. And, even when those records were available, they were not interactive. Information had to be extracted from the old record and entered into the new record. And as mentioned, if the patient had been seen, evaluated and treated fifteen times since the last hospitalization, none of those treatment events was available.
Not so, with SETMA. Every encounter, hospital, ED, clinic, all SETMA clinics, physical therapy, etc., are available to the provider who is assessing the patient. All of SETMA’s patients’ records are instantly available where ever our patients are being treated and particularly in the emergency department and in the hospital in-patient setting. That means that there is continuity of care between the ambulatory setting and the ED and inpatient settings, based on the documentation of the patient’s health care in the past. Medications, diagnoses, treatment plans and plans of care, laboratory data, and physician plans and consultations notes are all instantly available.
Rarely is a SETMA patient seen in the ED or hospital where the patient has not already had an exhaustive and established diagnoses and plan of care in the clinic. In addition, the EMR has 29 sets of guidelines for care and each patient has a physician-determined treatment plan in the EMR which plans are easily accessed by any and all SETMA providers. When the ER physician diagnoses CHF, SETMA has a treatment plan already written for the excellent and expert treatment of CHF. This is true of COPD, Pneumonia, Respiratory Failure, etc. Even the treatment orders, which are based on a physician’s diagnoses, are produced by electronic algorithms which are vetted by experts and embedded in our EMR.
For those patients who are new to SETMA, the diagnostic assessment and the treatment plan is initially determined by the ED physician and not by SETMA’s RN. There is always a SETMA physician available and typically one is in the hospital until 8 or 10 PM and others come in to the hospital between 2 and 4 AM, leaving only 4 to 8 hours a day when a SETMA physician is not physically available for patient care and collaboration with the SETMA nursing staff either in a personal “huddle” or in an “electronic huddle” by telephone or secure e-mail.
One of the elements of Patient-Centered Medical Home is a “huddle” where a team of providers meet daily to discuss a patient’s care. SETMA is introducing the world to “electronic huddles” made up of multiple communications daily:
- Morning notes electronically generated and submitted to the hospital care team daily. These notes give guidance to SETMA’s staff who work in the hospital around the clock to provide continuity of care and quality care to all of SETMA’s patients.
- iPhone contacts repeatedly during the day and night. The ability for nursing staff to communicate detailed notes, procedure results or x-ray and lab reports, adds to the continuity of care and to the rapidity with which information is communicated to the entire healthcare team.
- Secure e-mail allows procedure and test results to be communicated to the provider by the hospital staff allowing adjustments to treatment and initiation of new treatments to occur continuously all day and night.
- Electronic consultations with consultants and/or specialists can be done efficiently and timely.
Rather than a single point of care once a day, SETMA’s patients receive multiple points of care, multiple times a day, all initiated by physicians and all carried out by members of SETMA’s team. SETMA’s Model of Care has more physicians and more team member interacting on more patients every day than in any other model. The reality is that with multiple “sets of eyes” on a patient’s care, patient safety goes up as it is not unusual for experienced and knowledgeable RNs to bring an issue to the physicians’ attention which has not been addressed. The physician then gives instructions as how to respond but the real credit belongs to the nurse. This is only one example as to how the team increases the patient’s quality of and safety of care. RNs are not being asked or even allowed to operate outside of their licensure, but they are a dynamic and essential part of the healthcare delivery team.
On admission, after the history and physical examination is reviewed and approved by the physician, every patient admitted to SETMA receives a Hospital Plan of Care, which is a printed, personalized record of the patient’s diagnoses, consultations, procedures, tests, how long the patient is expected to be in the hospital, the probability of readmission upon discharge, a reconciled medication list and a precise explanation of how to contact both the admitting and attending physician and SETMA’s hospital support team This is in keeping with the PC-MH Model where our “electronic huddles” even involve the patients and their family.
In April, 2013, SETMA continued to think about this and published the following article: http://jameslhollymd.com/Your-Life-Your-Health/The-Future-of-Collaboration-Between-Physicians-and-Nurses.
Michael Fasher, MD is a General Practitioner and Adjunct Associate Professor University of Sydney and Conjoint Associate Professor University of Western Sydney. He and a team of physicians visited SETMA in March, 2014. After this visit, he said:
“I know I speak for all of us in thanking you and your team for your investment of time, financial and human resources in what for us was a horizon expanding and inspiring experience. Your technological expertise was no less breathtaking than the warmth of the relationships you so quickly facilitated between each of us and yourself and the outstanding individuals that make up that part of your team we were so privileged to meet.
“We need time to reflect on the huge panorama that has opened up as a result of viewing the world from that mountain peak, Mt SETMA. With trepidation I contemplate the need to be up - reading and writing - like you at 4 am. For today I will reflect on ...
"Quality metrics have made us better healthcare providers. The public reporting of our performance of those metrics has made us better clinician/scientist. But what makes us better healthcare providers is our caring for people."
“We recognize that the only way we can truly thank you is ..."" continued dialogue will stimulate both/[all] of us to excellence and to the transforming of health care delivery" Yours in astonishment and delight On behalf of the Team from Down Under”
In response to a note in October, 2015, Dr. Fasher said: “Perfect evidence to support our energetic advocacy for SETMA as being a light on the hill ever since our visit. Larry, our visit and your generosity as host was transformative. We are working away in western Sydney since our visit inspired by your moral imperative.”
The expansion of this reply originated when I spoke to the Massachusetts Medical Society in Boston; the following is a link to the full discussion: http://jameslhollymd.com/your-life-your-health/process-analysis-and-how-many-tasks-can-you-get-a-provider-to-perform-at-each-encounter. I will summarize some of it.
The application of this experience is that the three limitations to primary providers completing tasks are time, energy and value. In the Boston meeting, there were three speakers, each had an hour to speak and I was the last speaker. The first speaker asked, “How many tasks can you get a healthcare provider to perform at every patient encounter?” A vigorous discussion ensued at the end of which the speaker said, “I think you can get providers to do one thing.”
As the last speaker, I began by saying, “I would like to answer the first speaker’s question, but to do so, you must first answer the following questions”:
- How important is the task you are asking providers to do?
- How much time does it take?
- How much energy does it take?
If you were to create a formula to represent this process, there would be a direct correlation between how many tasks a provider can or will do and how important the tasks are; the more important the tasks, the more tasks a provider will do. There would be an inverse relationship between how much time it takes and how many tasks will be done; the more time it takes, the fewer tasks will be done. There would also be an inverse relationship between how much energy it takes and how many tasks will be done; the more energy it takes, the fewer tasks will be done.
The key to getting more done is to determine what is important and only to do that, and then to make the completion of the important tasks require less energy and less time. Let me illustrate. The Texas State Health Department’s Reportable Conditions illustrates the standardization and the automation of parts of healthcare processes. Remember Peter Senge’s statement in The Fifth Discipline: “The more complex a problem is, the more systemic the solution must be.”
After the below discussion, which shows that with electronics, many complex and important tasks can be reduced to one second, or no seconds, with little energy expenditure, In he Boston discussion, I concluded: it is possible to get providers to do thirty or forty things every time they see a patient and at SETMA we do.
How can healthcare providers design a solution to a complex healthcare problem, particularly when the problem is not generated by a patient’s request but by a public-health need? In the former case, the provider simply determines if the request is appropriate or not. In the latter case, no one is in the provider’s office requesting a service; a requirement has been established and it is up to the provider, in the midst of many other demands, to remember and to fulfill the requirement. In the case of infectious diseases, requirements have been published for providers to report the occurrence of dozens of conditions.
| Problem: |
The medical literature is filled with reports of a very low compliance of physicians with reporting infectious diseases to State Health Departments. In Texas, there are 78 infectious diseases which require reporting. The window for reporting compliantly varies from immediate, to one working day, to one week, to ten days, to one month. It is improbable that many healthcare providers know the entire list or the requirement for reporting. The Department of Health wants the report to be triggered by a suspicion and not by a confirmed diagnosis. If the provider waits until the confirmation is made, the opportunity for a public health intervention is lost. |
|
| Solution: |
A systems solution would be best. The ideal solution would be an electronic medical record (EMR) system in which the reporting action is triggered by the documentation of the diagnoses in the assessment in the EMR. |
|
| Scenario: |
On April 30, 2011, Dr. Holly made a presentation for a CME program at Texas A&M College of Medicine. The lecturer who followed him was Dr. Edward J. Sherwood, who lectured on “The Ethics of Infectious Disease.” Dr. Sherwood distributed a publication of the Texas State Health Department which detailed the 78 reportable conditions. |
SETMA’s IT Department was charged with designing a functionality which would:
- Display the reportable conditions for provider review
- Detail the time frame in which each infectious disease should be reported.
- Denote on the display of the reportable conditions the infectious disease which is identified by the provider. This would be done automatically when the diagnosis is documented on the assessment template in the EMR.
- Simultaneous with number three, a telephone message would be sent to SETMA’s Care Coordination which would then make the call or send the fax to report the infectious disease. The fact that this had been done will be stored in the EMR in a searchable fashion.
The same principles apply to the hospital. Few things represent the power of a team as SETMA’s history in the hospital. Since January 1, 2007, SETMA has discharged 18,952 distinct patients from the hospital, which represents 39,340 distinct instances of discharges/encounters as of today. That is an average of 2,000 distinct patients a year and 4,371 annual admissions. The Hospital Care Summary and the Post Hospital Plan of Care and Treatment Plan (the discharge summary—this name was changed at an NQF, Transitions of Care conference in September, 2010) was completed at the time of discharge on 96.5 percent of the discharges/encounters at the time of the discharge. I would like the percentage to be higher but this is not a bad number. For the hospital, this means no “held charges,” and effective transitions of care with all follow-up care, medication reconciliations and readmission risks determined before the patients leave the hospital. This is not the work of solitary physicians working by themselves but it is the work of a team.
In the same way, SETMA publicly reports on quality metrics by provider name on Care Transitions standards. On December 31, 2015, SETMA will complete seven years of quality metric audits on Transitions of Care Standards.
- Those reports can be found at: http://jameslhollymd.com/public-reporting/public-reports-by-type.
- The tool for the completion of this reported is explained at: http://jameslhollymd.com/epm-tools/hospital-care-summary-and-post-hospital-plan-of-care-and-treatment-plan-tutorial.
- The standard of Care Transition is based on the data set published by the American Medical Associations Physician Consortium for Performance Improvement (PCPI) which can be reviewed at: http://jameslhollymd.com/epm-tools/Tutorial-Care-Transition
- Following discharge from the hospital, every patient receives a hospital follow-up call the first day following discharge. The tool for this is explained at: http://jameslhollymd.com/epm-tools/Tutorial-Hospital-Follow-up-Call. This call is a 12-30 minute care coaching call which creates an effective continuum of care from the hospital. The following are the percentage of successful completion of follow-up calls by SETMA Care Coordination Department:
- SETMA’s Care Transition program is explained in the following tutorial: http://jameslhollymd.com/epm-tools/Tutorial-Care-Transition.
- Several years ago, CMS started paying physicians for doing effective Care Transitions. SETMA does this effectively. The following tutorial explains that process: http://jameslhollymd.com/epm-tools/transition-of-care-management-code-tutorial.
- Before the patient leaves the hospital not only is the medication reconciliation done, but follow-up visits are scheduled.
SETMA audits the quality of care which we perform. One of the audits we do is looking for statistical differences between the care received by those who are not readmitted within thirty days and those that are. Only two measures influence readmissions: one is whether or not the patient received the care coaching call the day after admission and the second is whether the patient had an ambulatory follow-up visit within 72 hours of leaving the hospital. Once again, this is not the work of a solitary physician working alone; it is the work of a team.
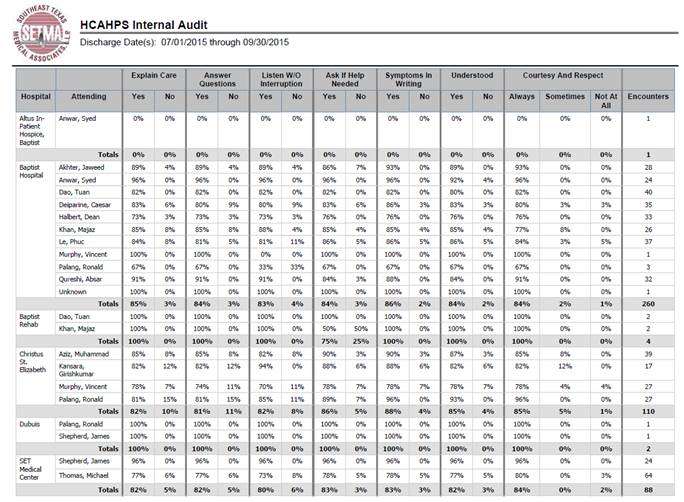
Patient Satisfaction is a critical part of provider and hospital responsibility today. Core Measures are also the current standard for measuring of the quality of provider/facility care of patients. Many providers are frustrated about being held accountable for standards which they do not know and about which they have heard. As a result, SETMA deployed information about core measures and HCAPHS.
The following is SETMA’s performance on HCAPHS as measured by our independent Care Coordination survey for one quarter; we have this for all quarters:
Again, SETMA’s performance on HCAPHS and Core Measures is a team function.
“I feel it is imperative for SETMA to give specific examples of how the RN taking call is able increase efficiency but yet remain compliant with the rules in the Nurse Practice Act.” (Amy Townsend, MD)
The first eighteen pages of this document establishes how deeply engrained into SETMA’s culture are:
- A team approach and even a team psychology
- Respect and admiration for registered nurses, nurse practitioners and other members of the healthcare team
- The depth and breath of tasks which SETMA requires of each provider, tasks which no solitary individual can possibly fulfill
First, let me correct Dr. Townsend’s implication that nurses are “taking call.” They are not; they are “screening calls” for efficiency, even when the doctor is in the hospital. Second, Dr. Townsend in classic argumentation and debate style has now included LVNs in the discussion when we have all already determined that LVNs have no place in the hospital. In order to try to win her argument, Dr. Townsend now says, “There is no difference between LVNs and RNs. The unspoken conclusion is that because we agree to exclude LVNs, which SETMA NEVER included, we must exclude RNs as they are no different from an LVN. That is irrational and would not be supported by the Texas Nursing Board.
The following are three questions and answers provided by someone - the answer sound like physicians who have small practices with a few calls at night and who have never managed a large, complex, healthcare system. They also sound like physicians who wish to impose their style of practice upon the entire medical staff without legal or medical justification.
- “They use protocols so that the physician does not get called.“ They batch calls so that physicians can get some sleep at night.”
MEC Response Nurse is using independent medical judgment when deciding how long to wait to call the physician - Dr. Holly’s comment: This is no different from the RN who places the call to the physician. The RN has made an “independent medical judgment” as to whether to call the doctor or not. Now that SETMA has a physician and/or a CFNP physically in the hospital all night this is a moot point but it will come up again when people who care about team work and transformation in healthcare are in charge rather than people who are still operating as if we are in the 1950s. If the answer given her is correct, I thing the MEC should require the hospital to hire physicians to be in-house who can review the care of each patient continuously so that no nurse is making any “independent medical judgment.” In fact, we should just eliminate nurses all together and hire physicians to give care to patients continually. This suggestion is no more excessive than the MECs note above.
- “a million calls about minor things like nausea or a fever”
MEC: Nurse is prescribing a therapeutic/corrective measures - see the following for the answer
MEC: Non-APNs/PAs cannot use protocols - Dr. Holly’s comment: Not sure where this rule comes from but it is not part of traditional medicine. Every order set has instructions which the nurse carries out such as frequency of vital signs, diets, activity, etc. These are treatment protocols. If the physician gives an as needed order with clear limiting parameters such as antiemetic for nausea, then the RN can execute that order without calling the physician to ask if it is OK to be done. If the hospital administration or the MEC wants to make that fundamental change in healthcare delivery, it will not withstand legal scrutiny and represents excessive intrusiveness by the MEC which seems to be driven by people who long for the way things were fifty years ago and are determined to resist progress.
- “I don’t need to talk to the ER physician about every admit. They can tell my nurse and I will see them in the morning.”
MEC: The decision to admit a patient is a joint decision between the ER physician and the admitting physician and requires independent medical judgment - Dr. Holly’s comment: The physician statement above is valid unless in the ER physician’s admitting judgment the patient needs to be seen immediately. The hospital by-laws does not require patients to be seen within twelve hours unless they are in ICU. Again, all of these answers seem to have been given by physicians who have chosen a style of practice which is personal and not required by excellent care and they are just trying to impose their choices on everyone else without legal or medical justification.
- Even when the doctor is in the hospital, the RN is able to receive a call, collect the information needed in order to answer the call and then either enter the doctor’s orders in the CPOE or CPOM or get the hospital nurse on the telephone so that the physician does not have to wait for the staff to find the nurse.
- Based on the review of SETMA’s Model of Care in the first twenty pages of this document, there are many tasks, internal to SETMA, but which are external to the hospital and which have value to the hospital, which the nurse can legitimately complete.
- The nurse can gather the laboratory results, procedure and radiology results to increase the efficiency of the provider.
- When the physician has seen the patient and completed his/her evaluation, the electronic medical record can be completed by the RN, can be signed by the physician and can be placed on the chart.
- All SETMA activities, external to the hospital, can be completed by the RN. Even in the case of sending medications to the pharmacy, the physician orders it and the RN can execute the electronic prescription. The RN can even place the information for electronic prescribing of narcotic into the EMR and then the physician with his/her identification can send the prescription. The RN cannot generate the six-digit code, put the physician’s personal code and send the prescription but up to those steps everything can be done by the RN.
- All of these activities contribute value to the hospital and to the patients care such as the Hospital Care Summary and Post Hospital Plan of Care and Treatment Plan being completed before the patient leaves the hospital and where the medication reconciliation, dictated by the physician, is completed in the EMR by the RN.
- Something as simple, yet as time consuming as which patients need to be seen and where they are, which is a simple but time consuming task, can increase efficiency. The RN also alerts the physician to any patients which have been overlooked. Simple? Yes, when you have one doctor and two admissions but when you have 47 providers and 28 admissions in a 24 hour period, it is complicated.
It should always be remembered, one size never fits all for all are never the same size. This does not only apply to numerical size but complexity of care model. SETMA demands a great deal of healthcare providers; with a team, it can be done, without a team it is impossible.
James (Larry) Holly, M.D.
C.E.O. SETMA
www.jameslhollymd.com
Adjunct Professor
Family & Community Medicine
University of Texas Health Science Center
San Antonio School of Medicine
Clinical Associate Professor
Department of Internal Medicine
School of Medicine
Texas A&M Health Science Center
|